05:00
Connecting residential segregation to non-communicable disease outcomes
EPID 684
Spatial Epidemiology
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
Today’s Theme
How can we appropriately measure the impacts of structural racism on spatial health inequality?
Agenda
Thoughts on the reading?
Take 2m on your own to take a look back at (1).
What struck you as interesting/confusing/frustrating?
What was interesting or surprising in reading this?
How does exposure to racial residential segregation impact cardiovascular disease (CVD) risk?
Kershaw et al. used longitudinal data from 2280 Black participants of a cohort study taking place from 4 cities.
Neighborhood-level intensity of exposure to segregation was a key input to the model.
Variation in systolic blood pressure was used as an indicator of CVD risk.
How might residential segregation impact CVD risk?
Stress
Access to medical care
Quality of overall physical environment.
Food access
And on, and on…
How can we measure individual-level exposure to segregation?
Measures like isolation, dissimilarity, centralization are all summaries of segregation or clustering in a given area.
Statistics like the Getis-Ord \(G_i^*\) allow us to capture local variation in exposure.
\(G_i\) is the predecessor to \(G_i^*\). Captures the same basic idea but is a bit more intutive.
Uses information on a location and its surrounding areas to estimate local intensity.
Getis-Ord \(G_i\) statistic
\[G_{i}(d)=\frac{\sum_{j}w_{ij}(d)x_j}{\sum_{j}x_j}\]
Where:
\(d\) is the maximum distance to consider clustering
\(w_{ij}(d)=1\) if place \(i\) and place \(j\) are within \(d\) of each other, and 0 otherwise. (When \(i=j\), \(w_{ij}=0\))
\(x_j\) is the variable of interest
Yields an estimate of both strength of clustering and approximate statistical significance.
Lets us go from this…
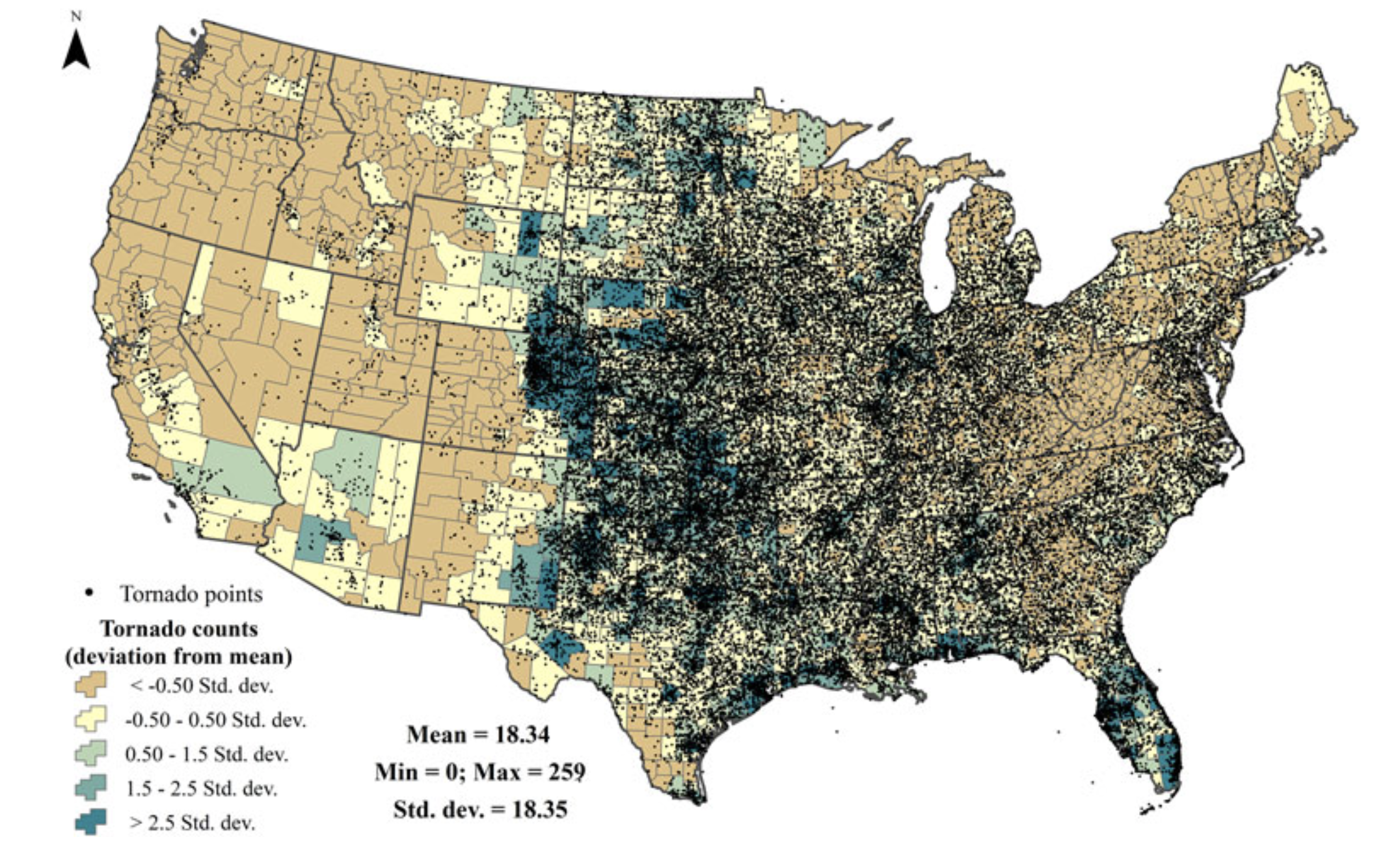
Tornado incidence from Frazier 2019
To this…
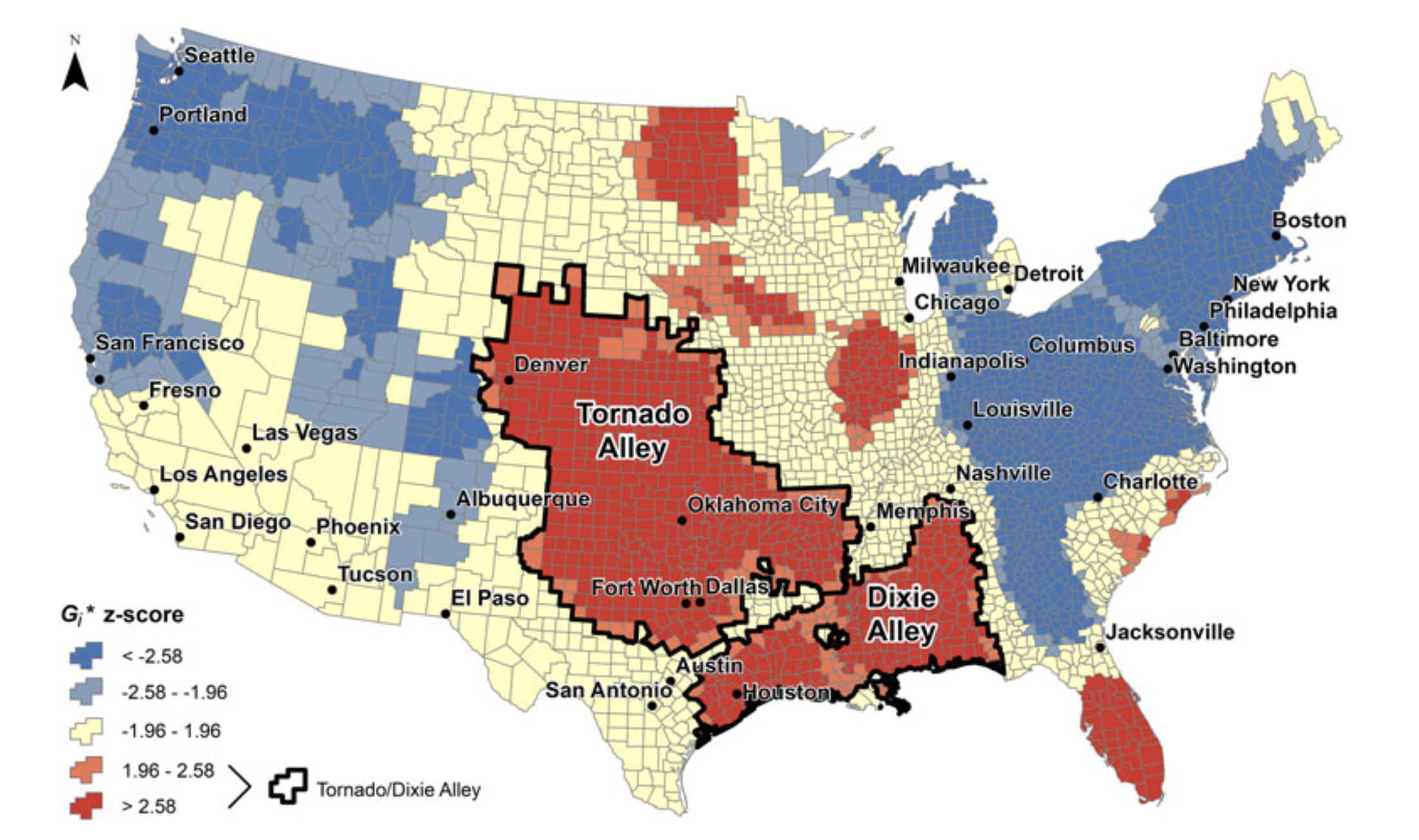
Tornado hot and cold spots identified in Frazier 2019
Long-term cohort design in Kershaw et al. allows study of within-person changes in exposure to segregation.
Allows adjustment for individual-level factors such as age, sex, physical activity, smoking, etc.
Can measure changes in segregation intensity in neighborhood of origin and destination for people who have moved.
Have to be sure that people who moved are not systematically different from those who didn’t.
Higher intensity of segregation \(\to\) higher blood pressure.
People who moved from a high- to lower-segregation context experienced small but meaningful decreases in blood pressure.
Suggests that policies facilitating neighborhood mobility could have positive health effects.
Reliance on SBP as a proxy for CVD is a limitation, but a common one when the outcome is relatively rare and the effect is subtle - even if it is important.
Comparing approaches
Take a few min to go back and re-familiarize yourself with the earlier readings.
As you’re doing this, add notes to this this Miro board to help distill/compare/contrast the approaches in each.
Add questions or points of confusion to the board as well.
Go beyond the readings as well to think about other types of spatially clustered exposures.
What are the characteristics of COPD?
Chronic inflammation of airways and alveoli.
Characterized by chronic cough and sputum production.
Severity of cough and sputum associated with worse COPD outcomes.
Increased risk of respiratory infection.
How does segregation impact COPD disparities?
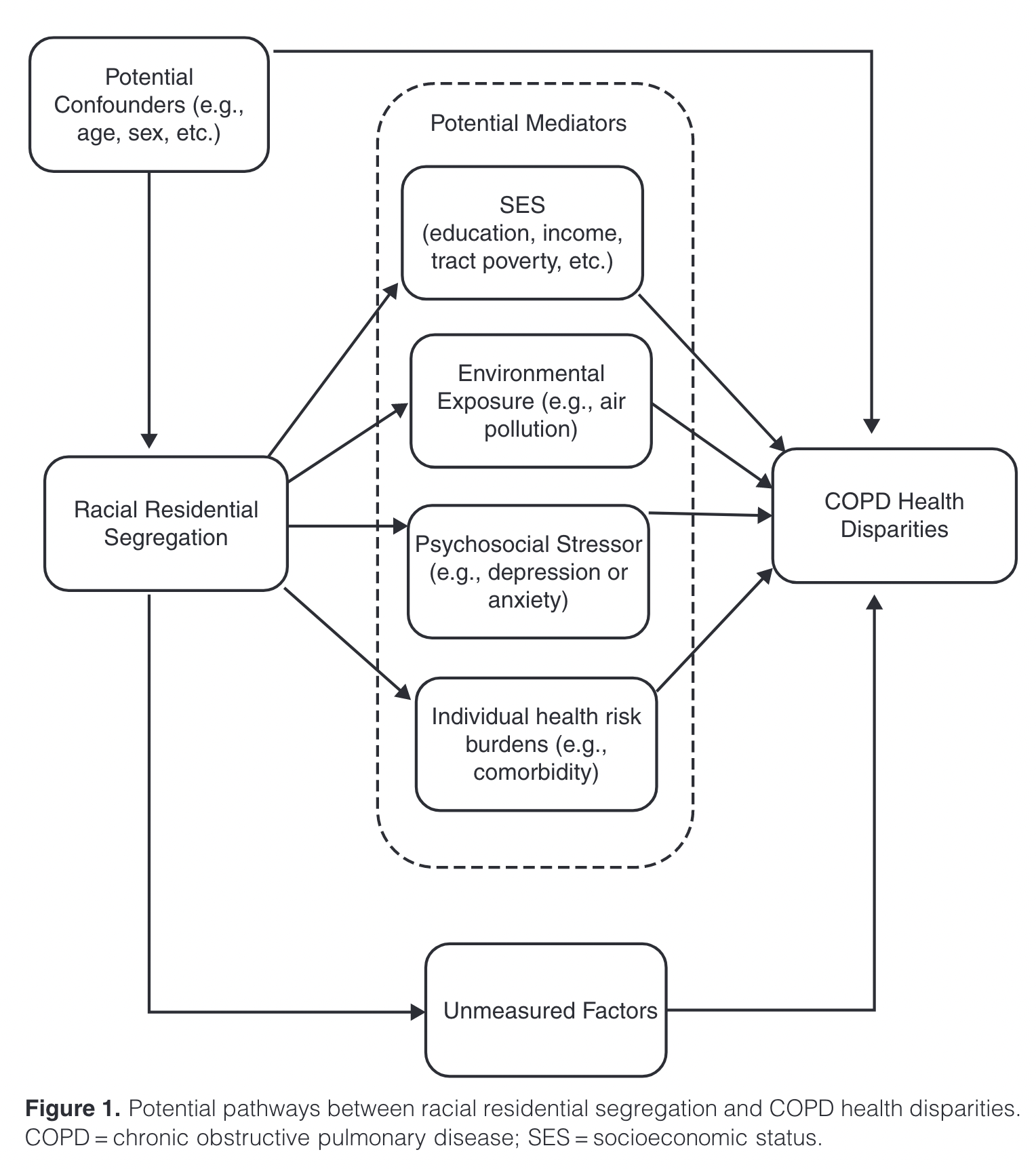
Relationships between segregation and COPD from (2)
Why is mediation analysis useful for understanding impact of segregation on health?
Segregation is a construct reflecting a complex mix of social and environmental factors.
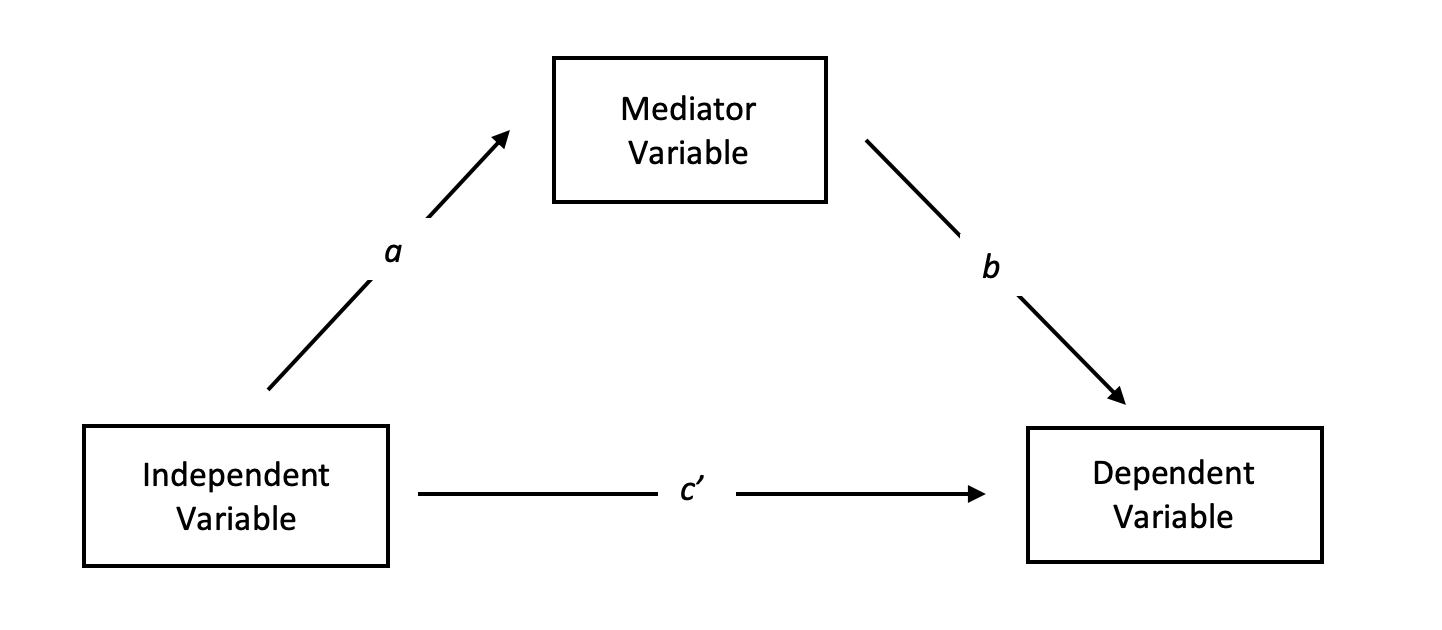
What does a mediation model measure?
Total effect: Relationship between distal factor and outcome including direct and indirect effects.
Direct effect: Relationship between distal factor and outcome adjusted for mediator.
Indirect effect: Impact of distal factor via a more proximal one.
In an additive model: indirect = total - direct
What might not sit right about this statement from (3)?
“Isolation may increase the risk for gonorrhea through its effect on social factors as well. Social norms — which also can be transmitted — have been shown to be associated with sexual risk among adolescents and among Black women. In isolated communities, within group norms for risky sexual behavior might be strengthened.” (3)
Next Time
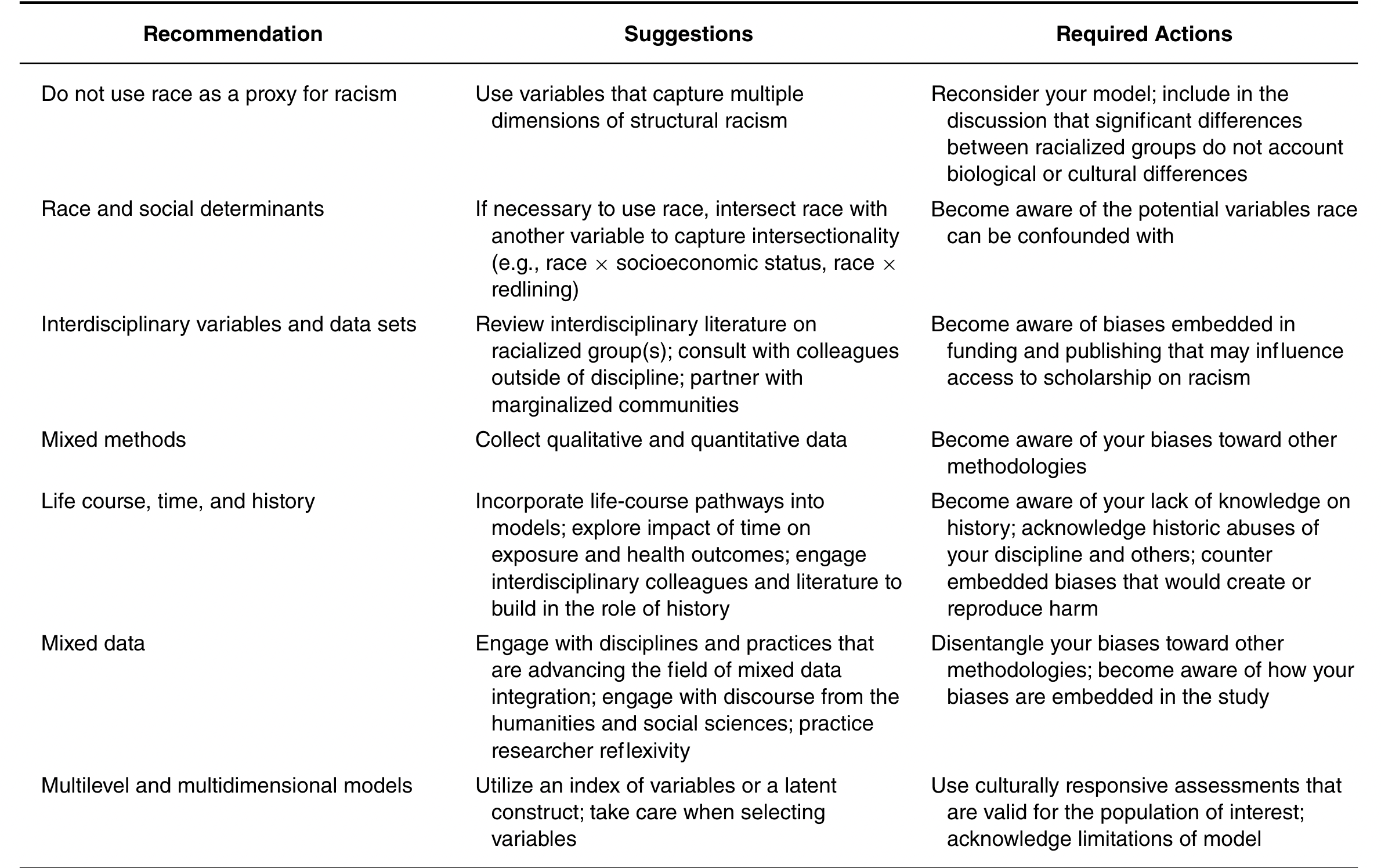
Suggestions for accurately measuring the nature of and impact of structural racism on health outcomes (From (4))
References
1.
Kershaw KN, Robinson WR, Gordon-Larsen P, et al. Association of Changes in Neighborhood-Level Racial Residential Segregation With Changes in Blood Pressure Among Black Adults: The CARDIA Study. JAMA Internal Medicine [electronic article]. 2017;177(7):996–1002. (https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2626858). (Accessed January 21, 2020)
2.
Woo H, Brigham EP, Allbright K, et al. Racial Segregation and Respiratory Outcomes among Urban Black Residents with and at Risk of Chronic Obstructive Pulmonary Disease. American Journal of Respiratory and Critical Care Medicine [electronic article]. 2021;204(5):536–545. (https://www-atsjournals-org.proxy.lib.umich.edu/doi/full/10.1164/rccm.202009-3721OC). (Accessed February 9, 2022)
3.
Biello KB, Kershaw T, Nelson R, et al. Racial Residential Segregation and Rates of Gonorrhea in the United States, 2003–2007. American Journal of Public Health [electronic article]. 2012;102(7):1370–1377. (http://ajph.aphapublications.org/doi/10.2105/AJPH.2011.300516). (Accessed December 15, 2019)
4.
Adkins-Jackson PB, Chantarat T, Bailey ZD, et al. Measuring Structural Racism: A Guide for Epidemiologists and Other Health Researchers. American Journal of Epidemiology [electronic article]. 2021;kwab239. (https://doi.org/10.1093/aje/kwab239). (Accessed February 8, 2022)