01:00
Modeling the fundamental causes of infection inequity
CDC Influenza Modeling Network Meeting
8/24/2023
Jon Zelner
[email protected]
Dept. of Epidemiology
Center for Social Epidemiology and Population Health
University of Michigan School of Public Health
EpiBayes Research Group
epibayes.io
![]()
TLDR
Why the fundamental social cause perspective is a powerful adjunct to mechanistic modeling.
Thinking through the implicaitons of a social causation framework for intervention and policy.
A very incomplete framework for equity-forward modeling.
There is nothing new under the sun ☀️
From Dubos (1955) (3)
During the COVID-19 pandemic, social causes of infection inequity were quickly identified
One of many examples of important insights that didn’t make it into early pandemic models. (4)
Historical analyses have repeatedly demonstrated how social structures drive infection inequities
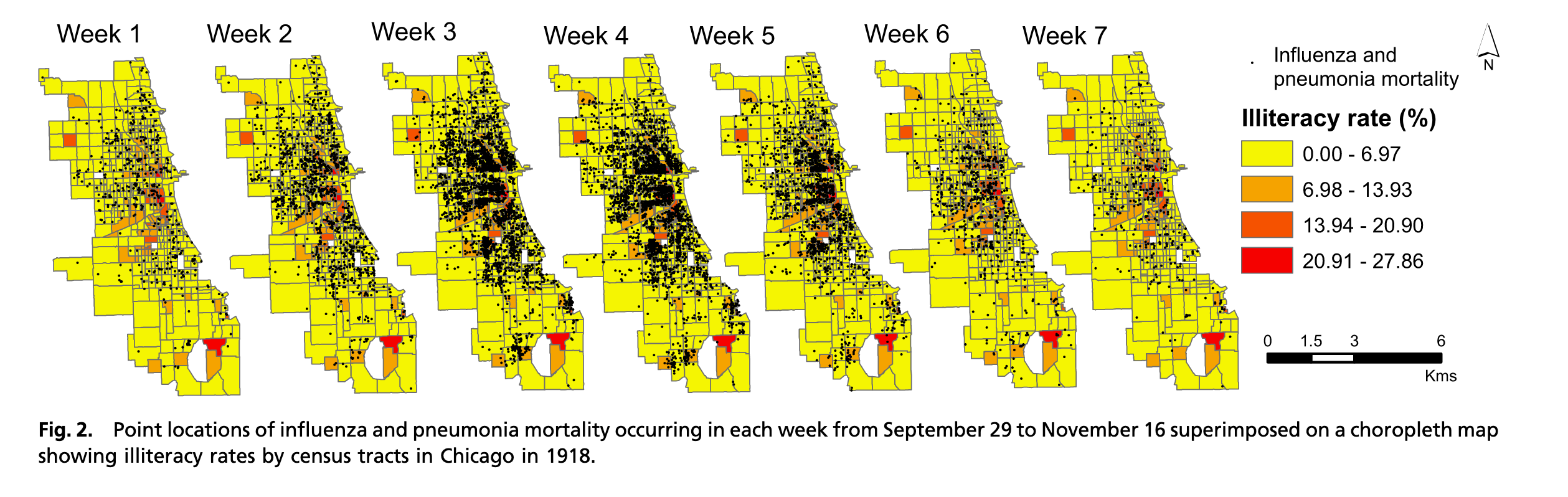
Example of spatial and racial inequities in 1918 influenza mortality from (5)
A lack theory, intuition, data, and methods for anticipating and targeting inequity was a signal failure of preparedness.
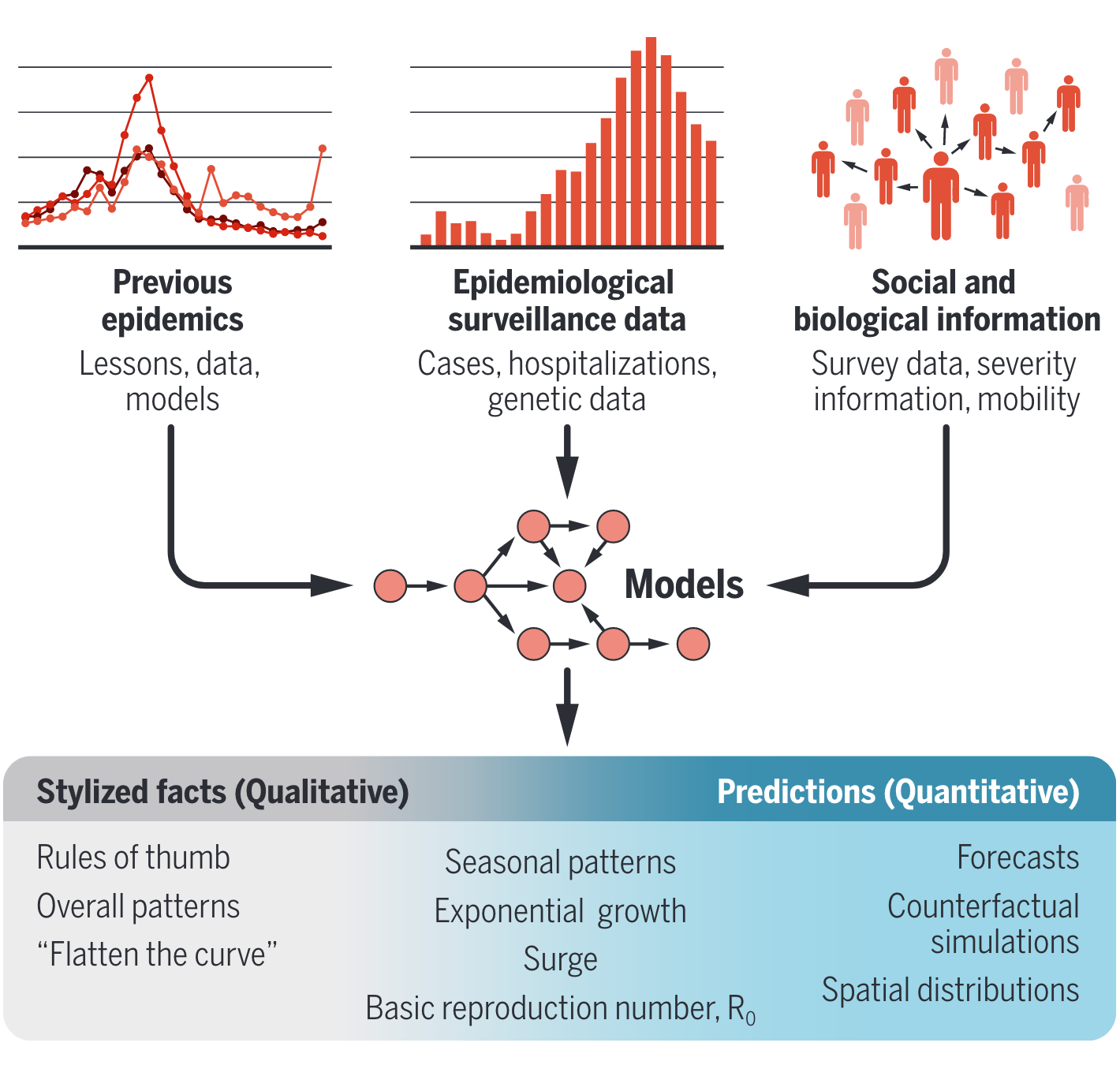
Implications of COVID-19 modeling have been broad, shaping everything from intuition, to public policy and social discource (Figure from (6))
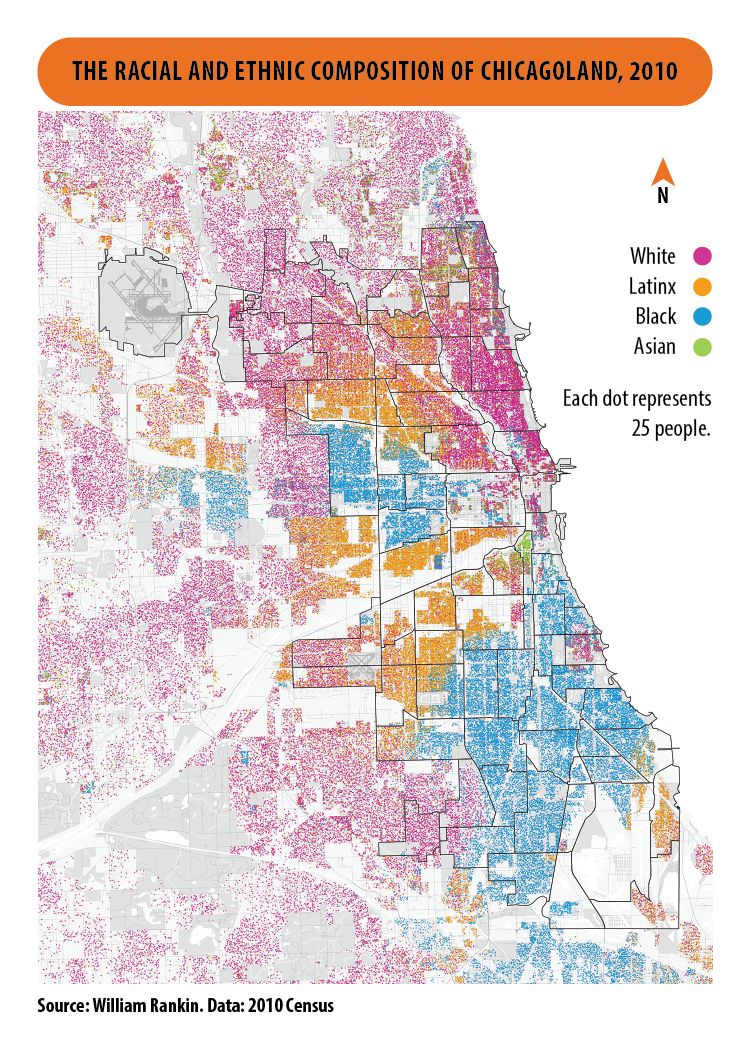
Structural determinants of unequal risk remain firmly in place
Occupational and residential segregation
Income and wealth inequality
Structural racism in public health, social policy, and medical practice
And too many other mechanisms to enumerate them all…
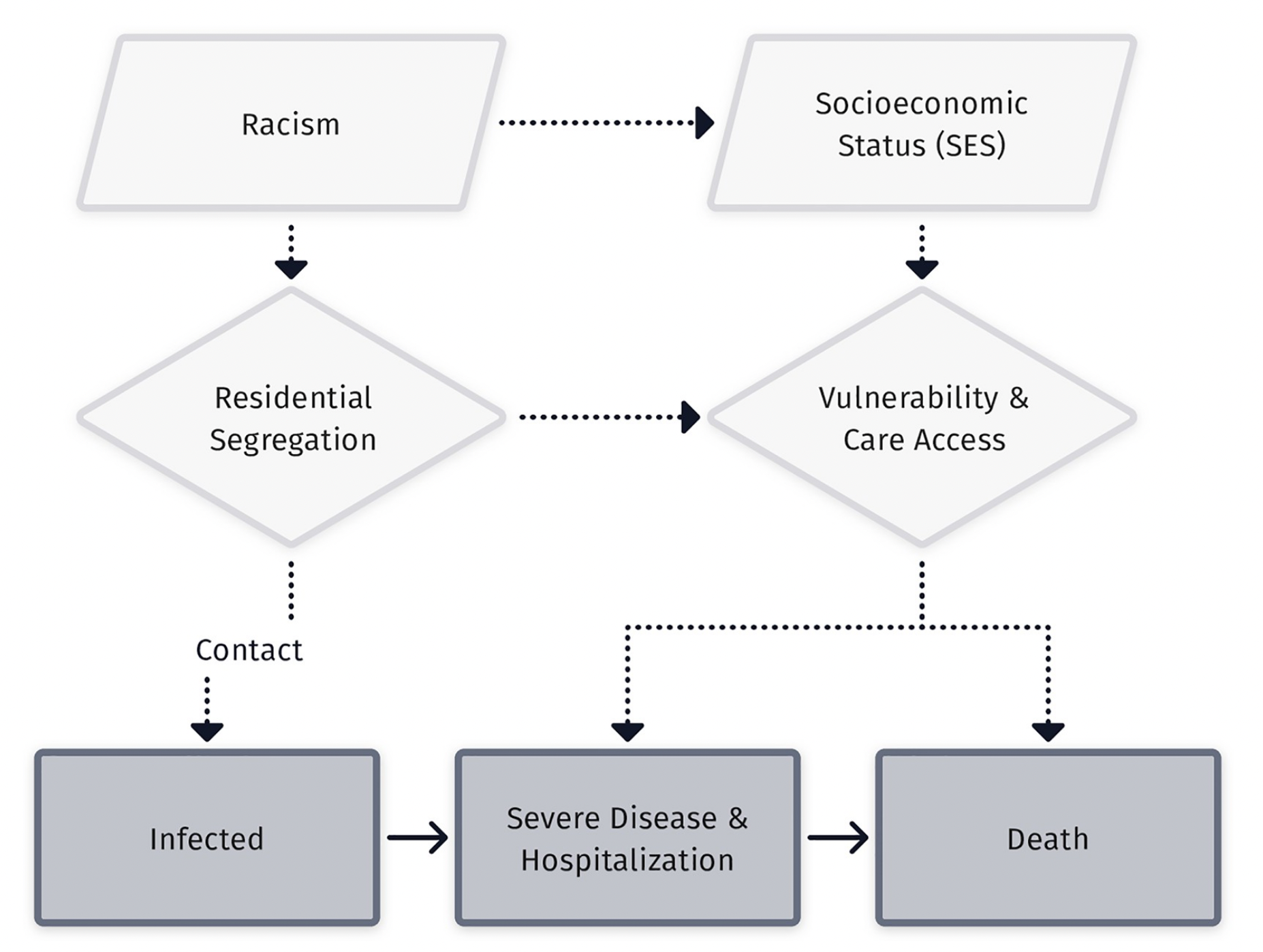
Fundamental causes such as racism are characterized by their pervasiveness and durability.
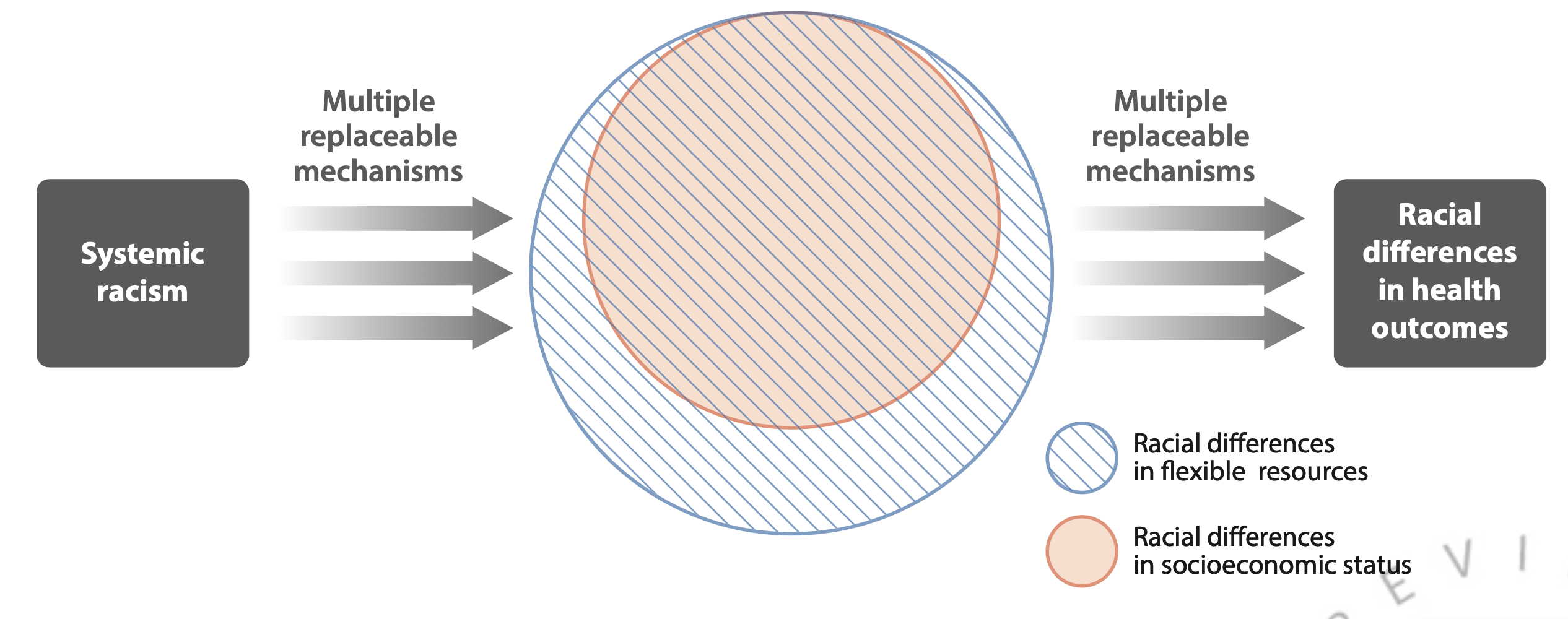
Theoretical diagram from (8) showing relationships between racism, socioeconomic inequity and racial inequity in disease outcomes.
FCT suggests there are diminishing returns to enumerating and attacking the mid-stream drivers of infection inequity
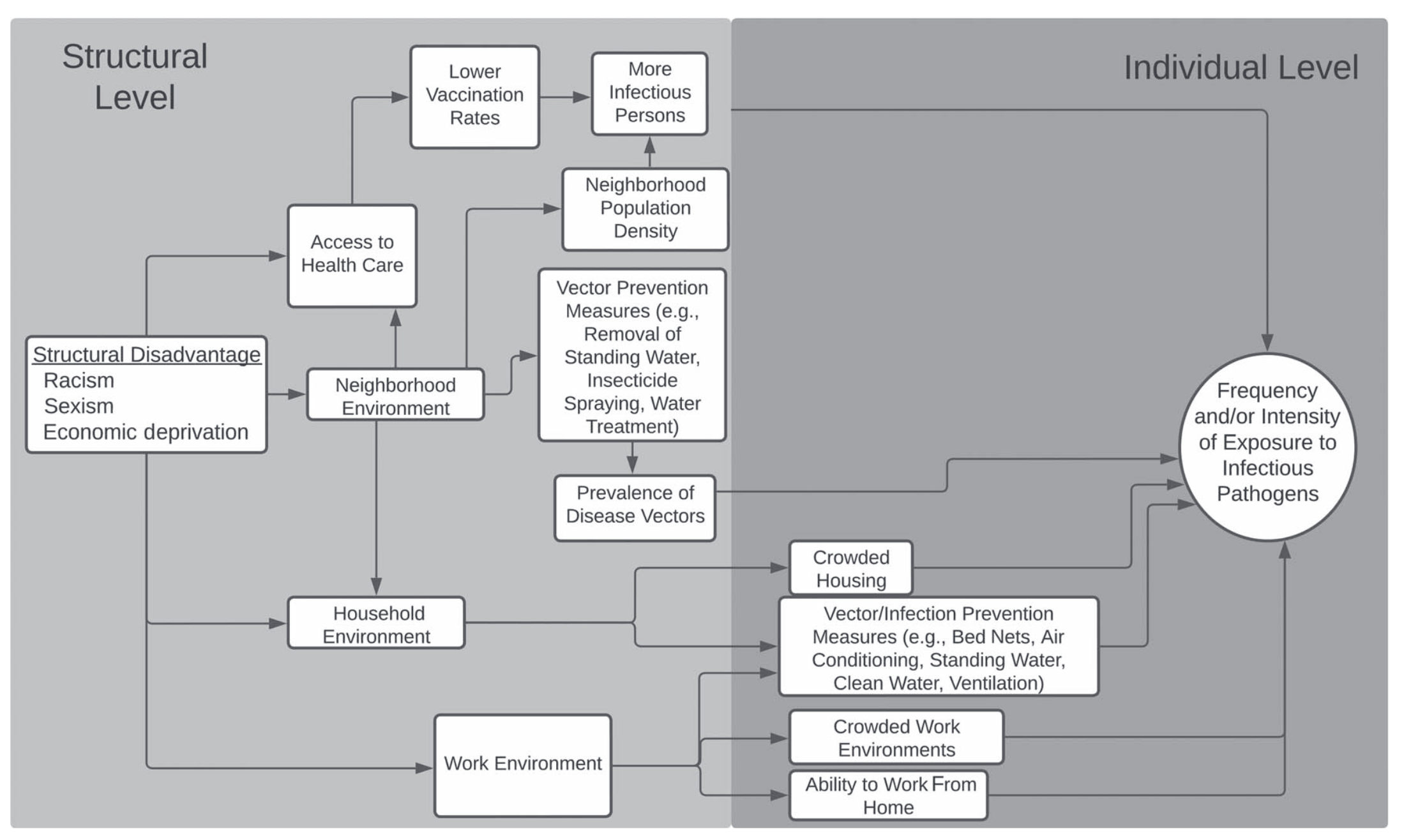
Flow diagram of connections between high-level, structural causes, intervening mechanisms, and downstream exposure risks, from (9)
FCT shows that innovation may result in increased inequity
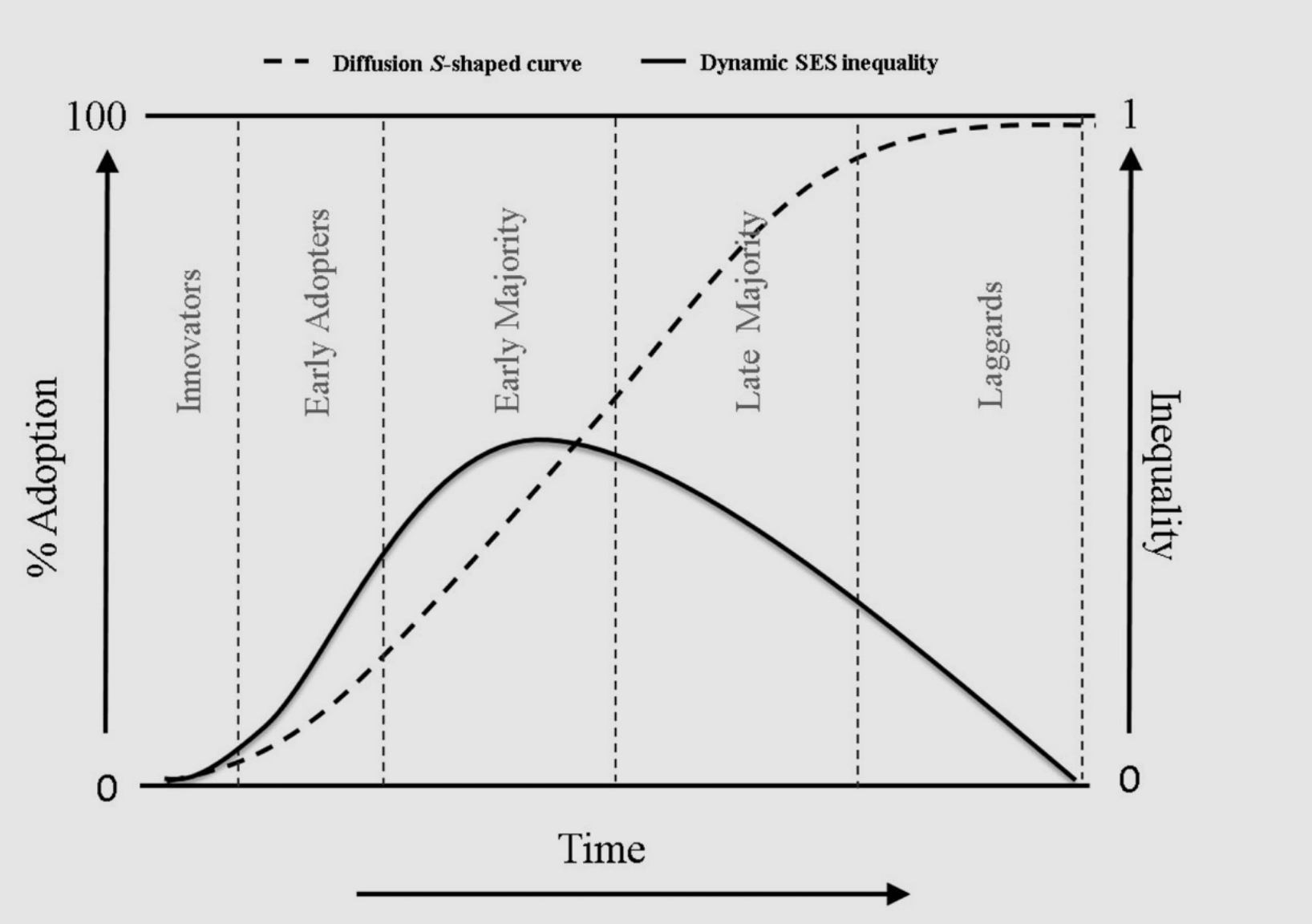
Diffusion of a new medical innovation through a population (dashed line) along a gradient of socioeconomic inequity (solid line) (Figure from Zapata-Moya 2019 (10); see also (11))
How does this play out in the real world?
Work-from home and other NPIs are also public-health innovations drive inequity.
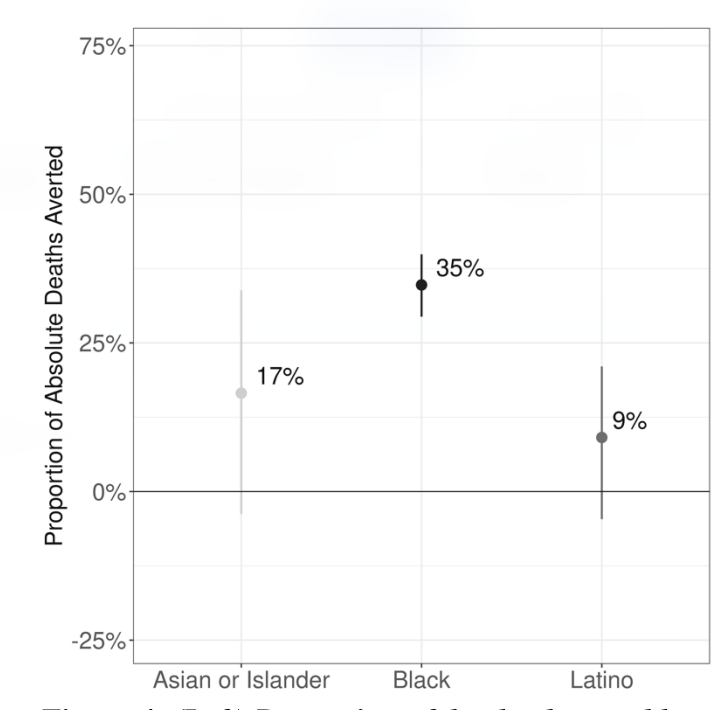
Proportion of SARS-CoV-2 deaths potentially averted in 2020 if all Michiganders experienced the same pacing of SARS-CoV-2 infection as Whites (From Naraharisetti et al., Under Review)
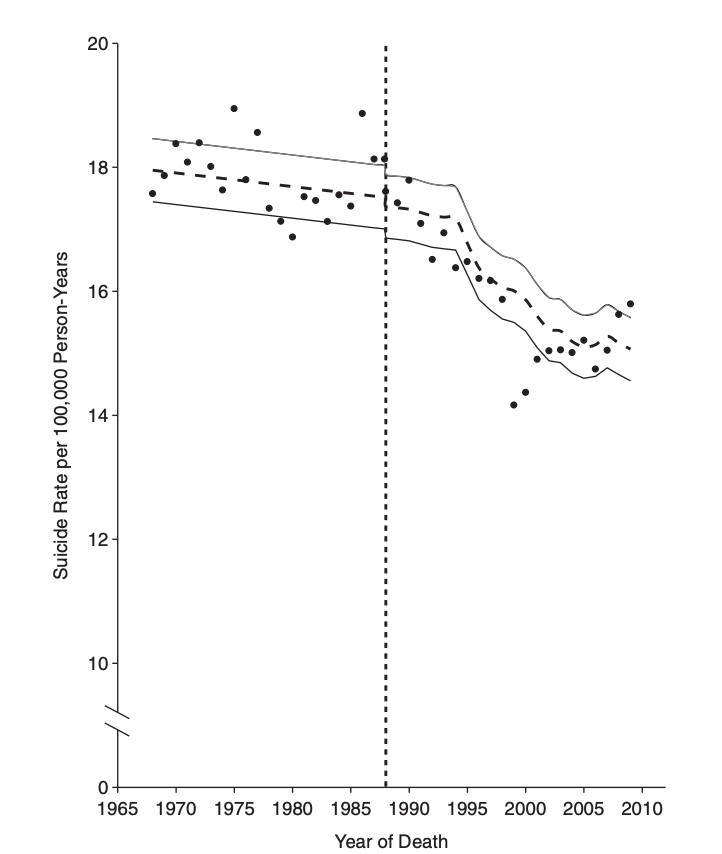
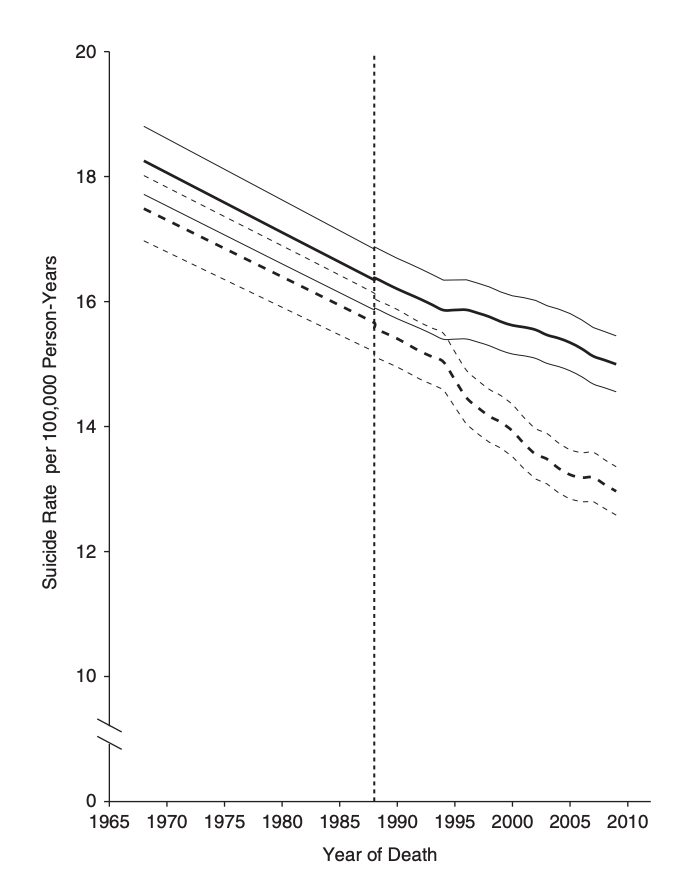
These patterns clearly in evidence during the roll-out of SARS-CoV-2 vaccine
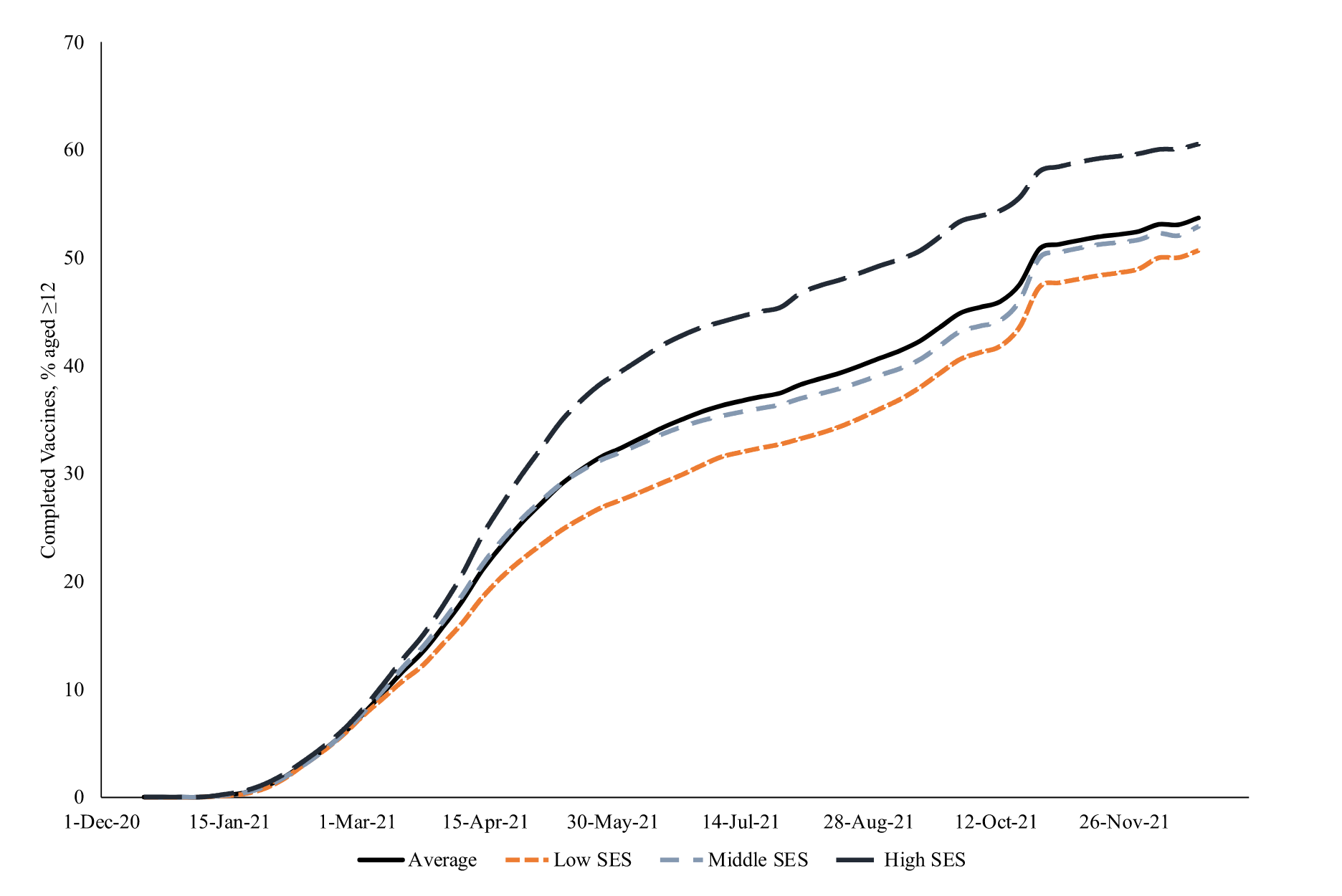
High-SES counties were vaccinated faster, earlier, and more completely than lower-SES counties (From Clouston et al. 2023 (13))
Can well-defined interventions remediate fundamental causes of infection inequity?
The only ‘well-defined intervention’ for racial disparities that can attack all of the pathways connecting structural racism to health inequity (as described by Richardson (16), with a healthy dose of irony)
We all know that being ready for the next emergency is not optional.
Recognize the embeddedness of models and modelers in sociopolitical systems
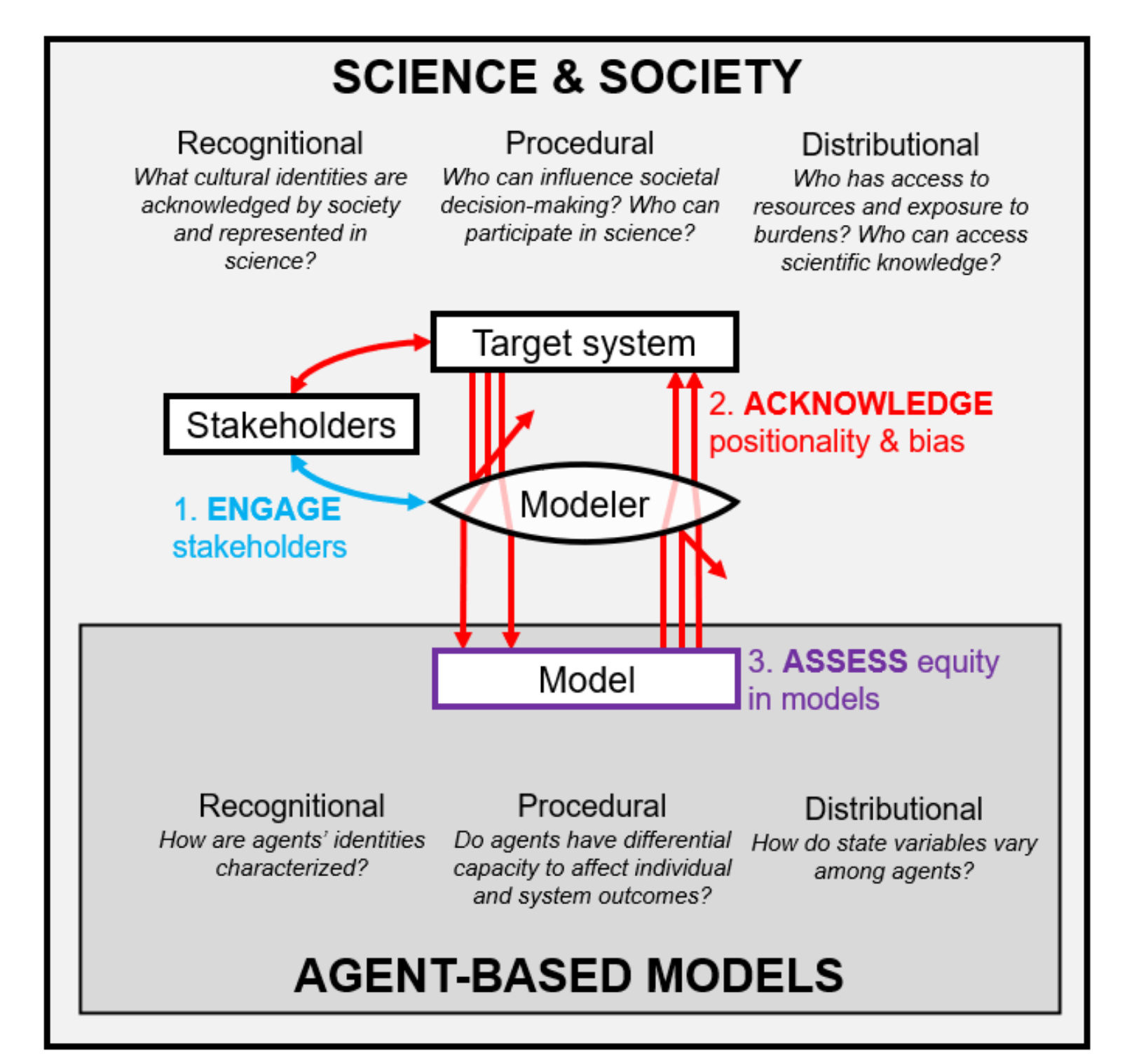
Example framework from Williams et al. (19) situating models and modelers within a system of social relationships and constraints.
Treat social and economic policies as first-line epidemiological interventions.
Examining the impact of ending the CDC eviction moratorium on COVID-19 infection inequity requires accounting for multiple levels of transmission (Figure from (20))
Highlight the distributional implications of existing social inequities.
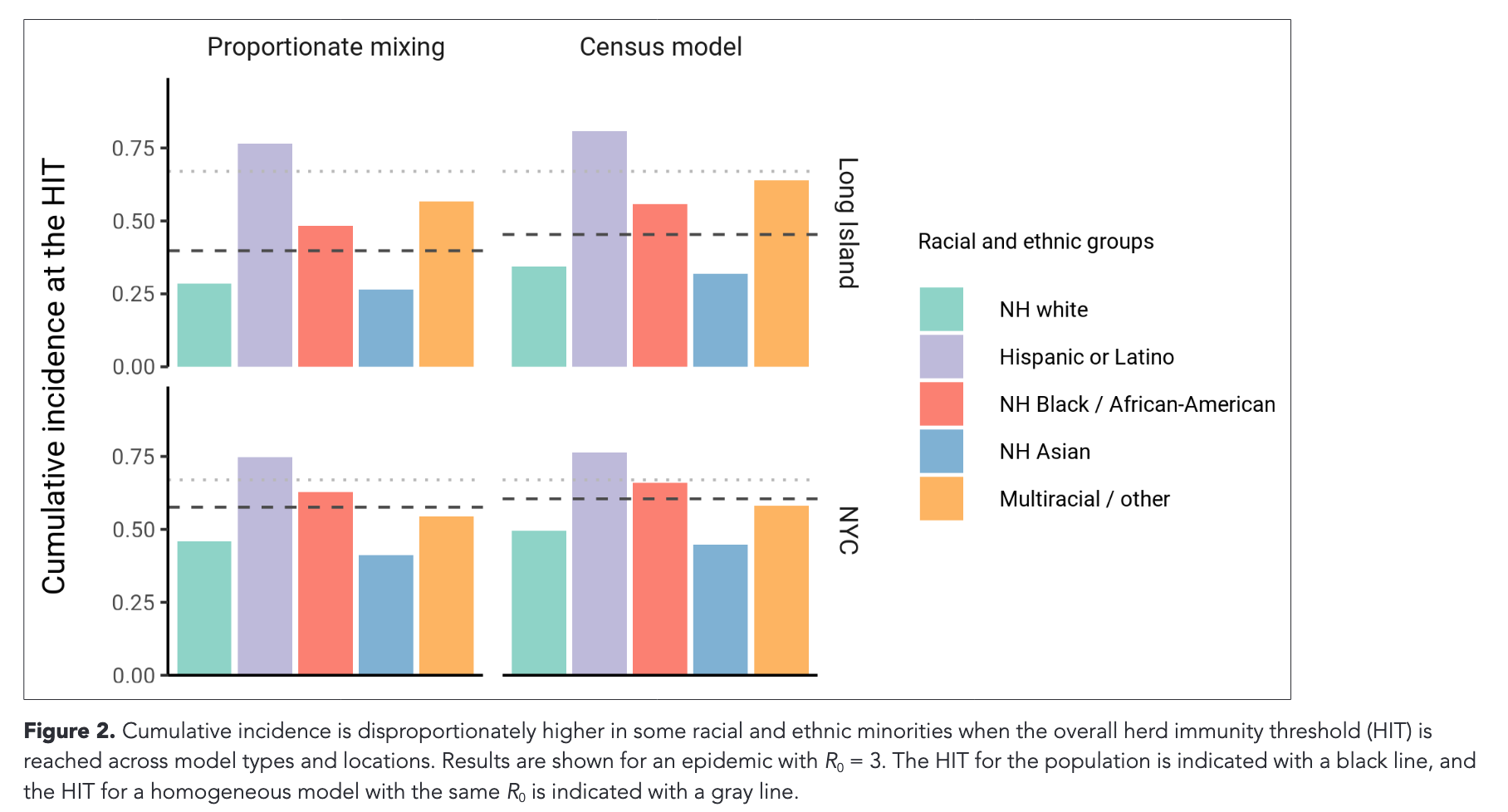
Example from Ma et al. (21) showing cumulative burdens of infection by race/ethnicity at a modeled herd immunity threshold for SARS-CoV-2
While paying attention to the balance between social and biological mechanisms as drivers of infection outcomes.
Casanova (24) points out ambiguities in Dubos’ ideas about ‘resistance’ and how modern immunology complicates simplistic ideas about the relationship between host and environment.