How should infectious disease models tackle infection inequity?
Jon Zelner
[email protected]
Dept. of Epidemiology
Center for Social Epidemiology and Population Health (CSEPH)
University of Michigan School of Public Health
EpiBayes Research Group
epibayes.io
![]()
Economic and racial inequity has been a central story of the COVID-19 pandemic





So why were we not prepared for these easy-to-foresee inequities?
Early-pandemic modeling infrastructure lacked theory, intuition, data, and methods for anticipating and targeting inequity
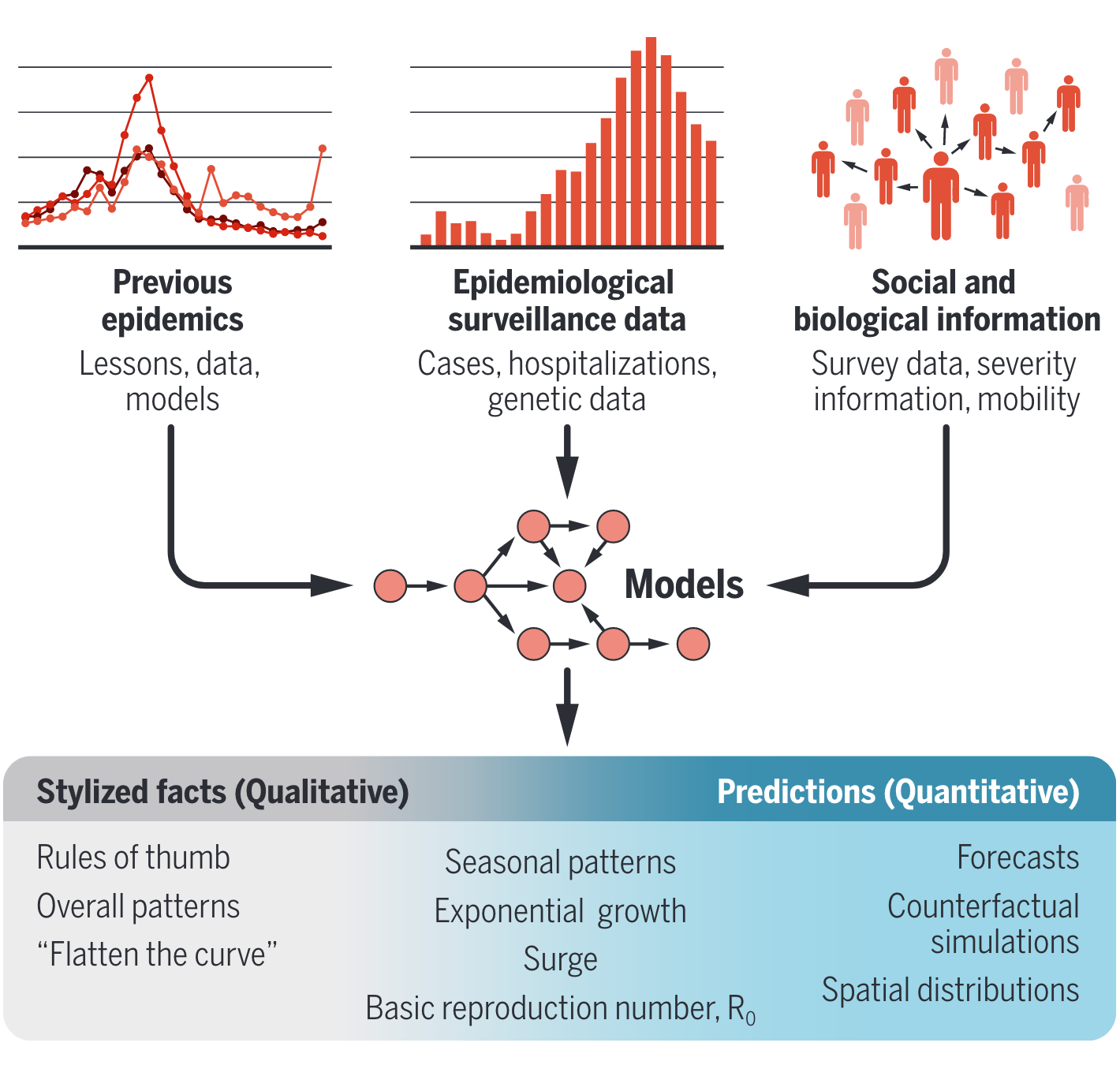
Implications of COVID-19 modeling have been broad, shaping everything from intuition, to public policy and social discource (Figure from (1))
The myth of the equal opportunity infector crowded out inequity as a central concern

What should an alternative approach account for?
- Model spatially localized infection risks as a function of upstream social determinants.
- Represent correlation between effects of factors such as racism and SES on spatial variation in infection risks.
- Examine differential impacts of social inequity on contact, susceptibility, and infectiousness.
Zelner et al. (2022), There are no equal opportunity infectors. PLOS Computational Biology
Equity-oriented models require a detailed understanding of the connections between high-level, intermediary, and proximal causes of infection
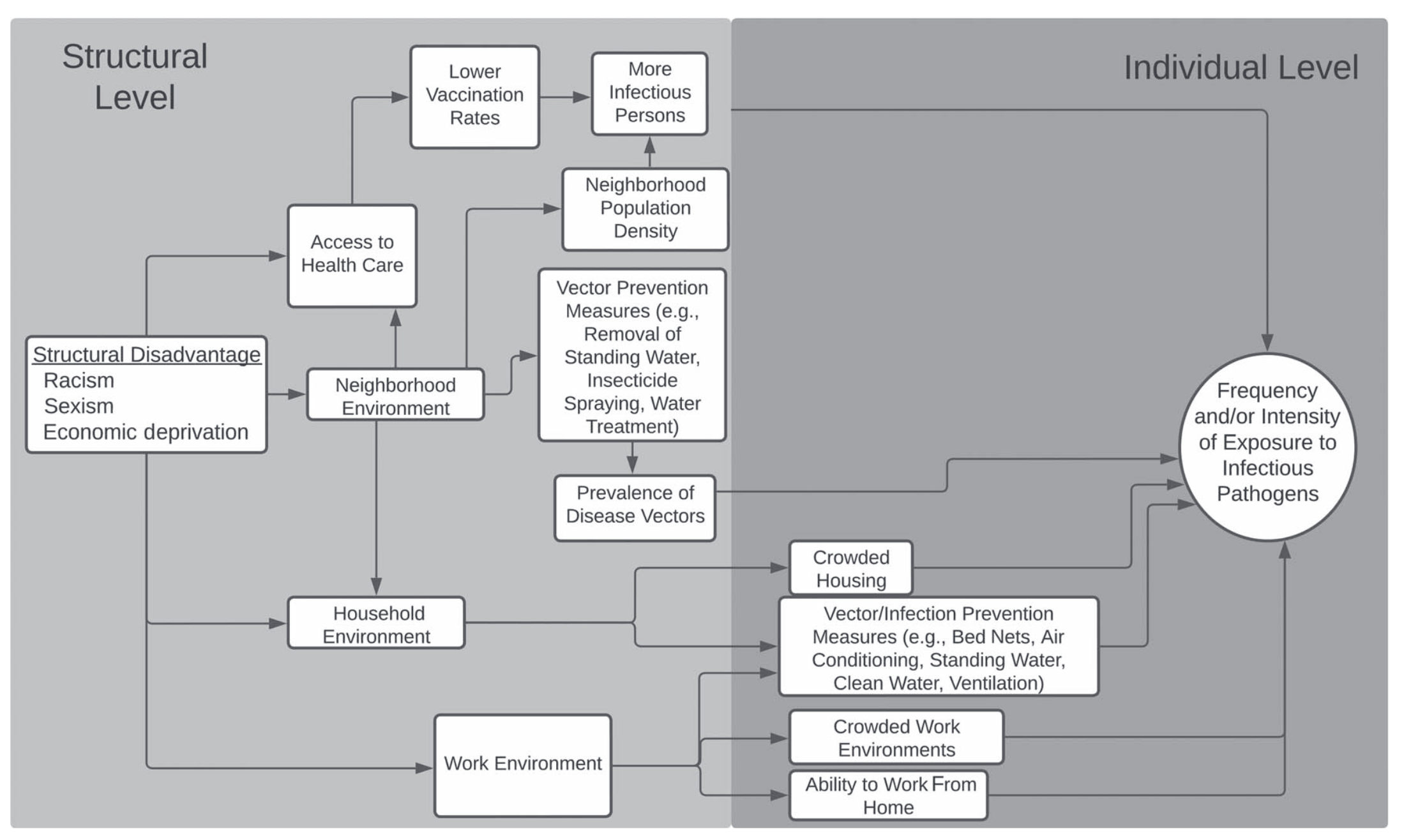
Flow diagram illustrating connections between high-level, structural causes, intervening mechanisms, and downstream exposure risks from (2)
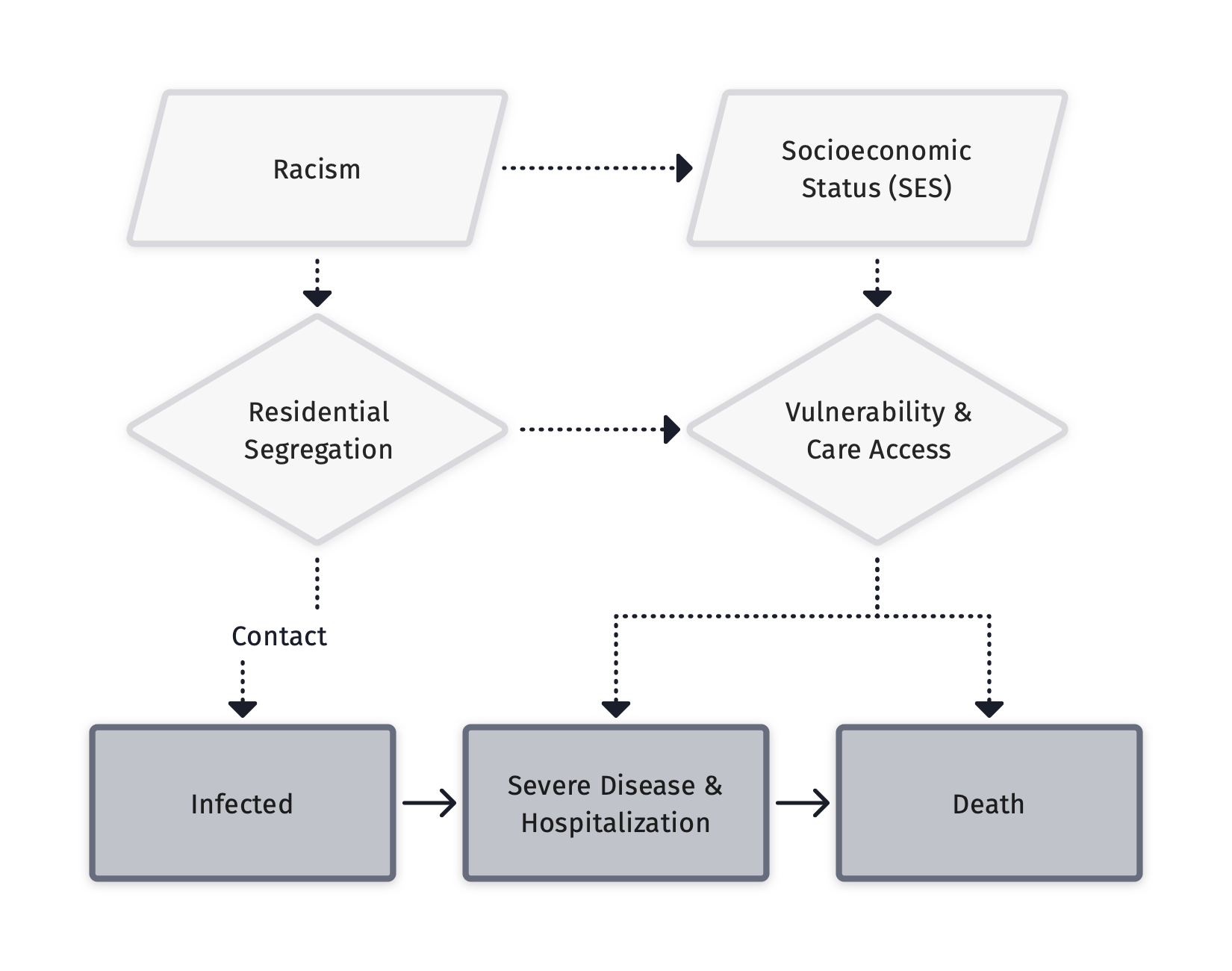
Equity-oriented models do not treat race as a causal variable
Theoretical diagram from (3) showing the complex relationship between racism, socioeconomic inequity and racial inequity in disease outxomes.
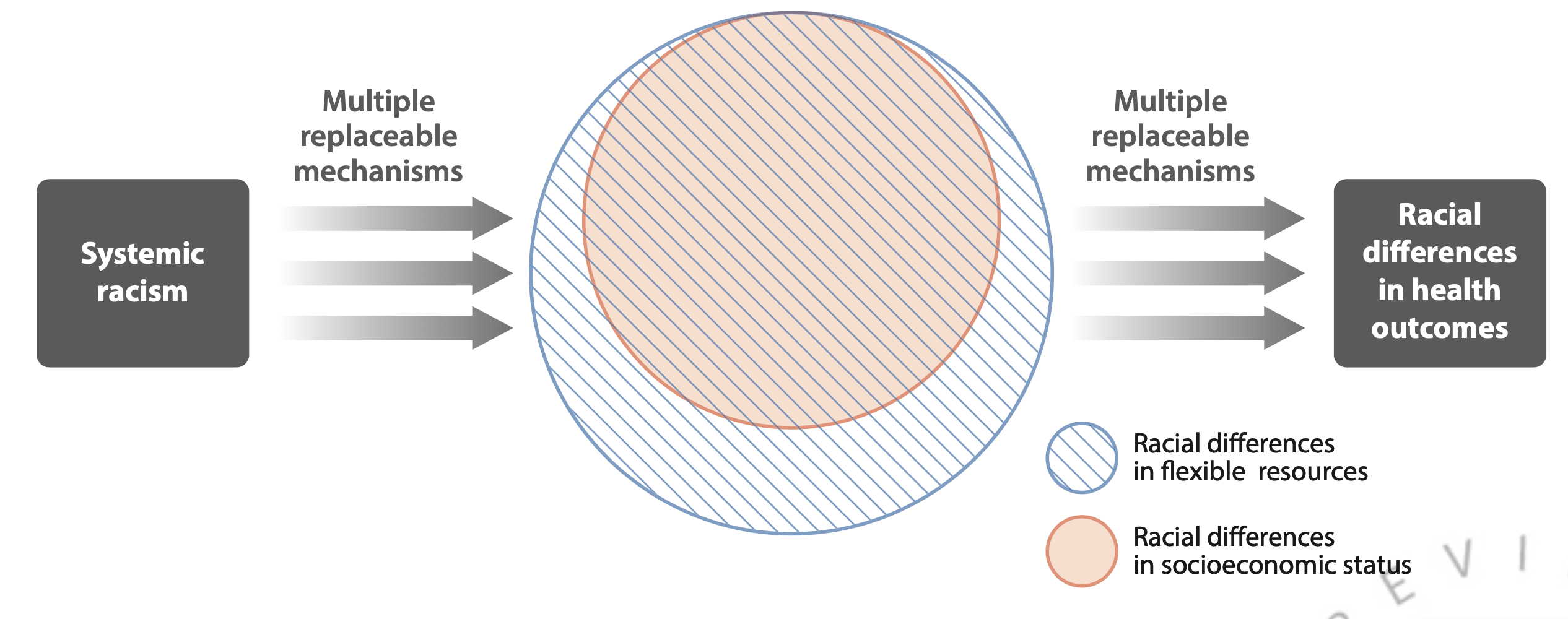
Equity-oriented models account for intersecting identities
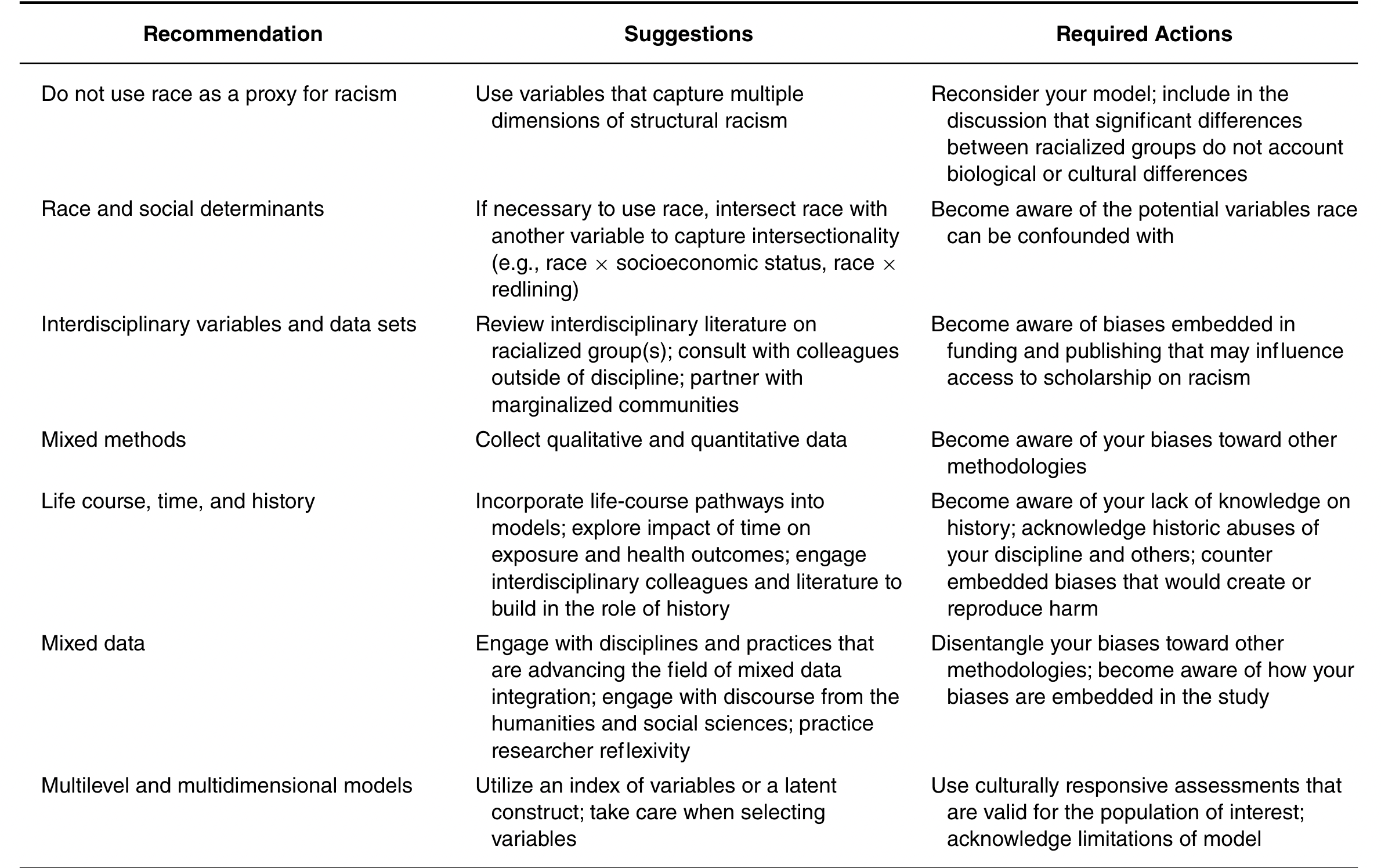
Suggestions for how to account for structural racism in epidemiological analyses from (4)
Equity-oriented models use contrasts that reflect structural change
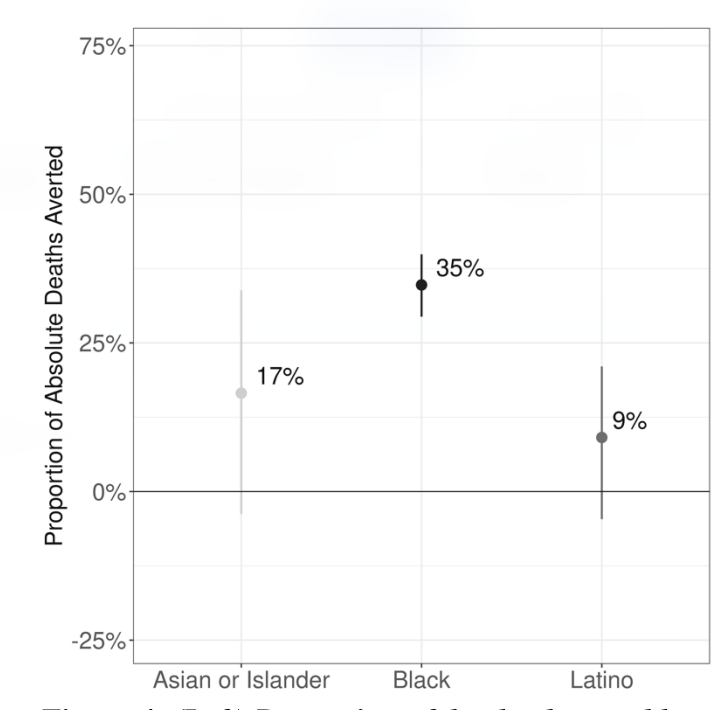
Proportion of SARS-CoV-2 deaths potentially averted in 2020 if all Michiganders experienced the same pacing of SARS-CoV-2 infection as Whites (From Naraharisetti et al., Under)
Equity-oriented models engage political questions
From Nande et al. “The effect of eviction moratoria on the transmission of SARS-CoV-2”, Nature Communications, 2021