There are no equal opportunity infectors
Making equity a first-class concern of epidemiological model(er)s.
2023 IDM Symposium
Jon Zelner
[email protected]
Dept. of Epidemiology
Center for Social Epidemiology and Population Health
University of Michigan School of Public Health
EpiBayes Research Group
epibayes.io
![]()
Inequity in COVID-19 death was easy to foresee, but most early models didn’t have much to say about it.





Effective vaccines and other interventions increased inequity even while decreasing overall risk

A lack theory, intuition, data, and methods for anticipating and targeting inequity was a signal failure of preparedness.
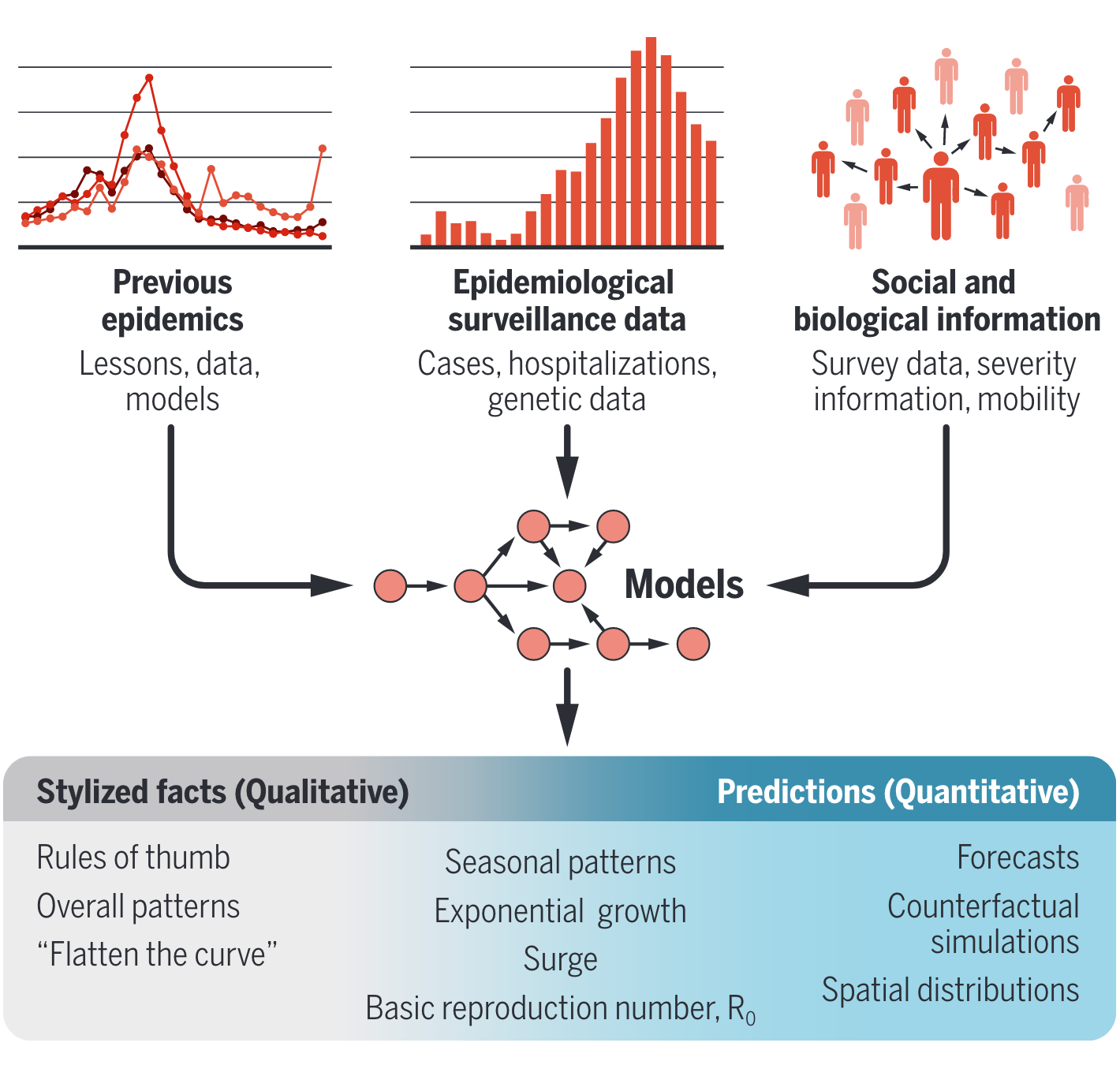
Implications of COVID-19 modeling have been broad, shaping everything from intuition, to public policy and social discource (Figure from (1))
Archetype of viral pandemics as equal opportunity infectors precluded socio-structural understandings of pandemic risk.

Equity-oriented models require an informed understanding of the connections between high-level, intermediary, and proximal causes of infection.
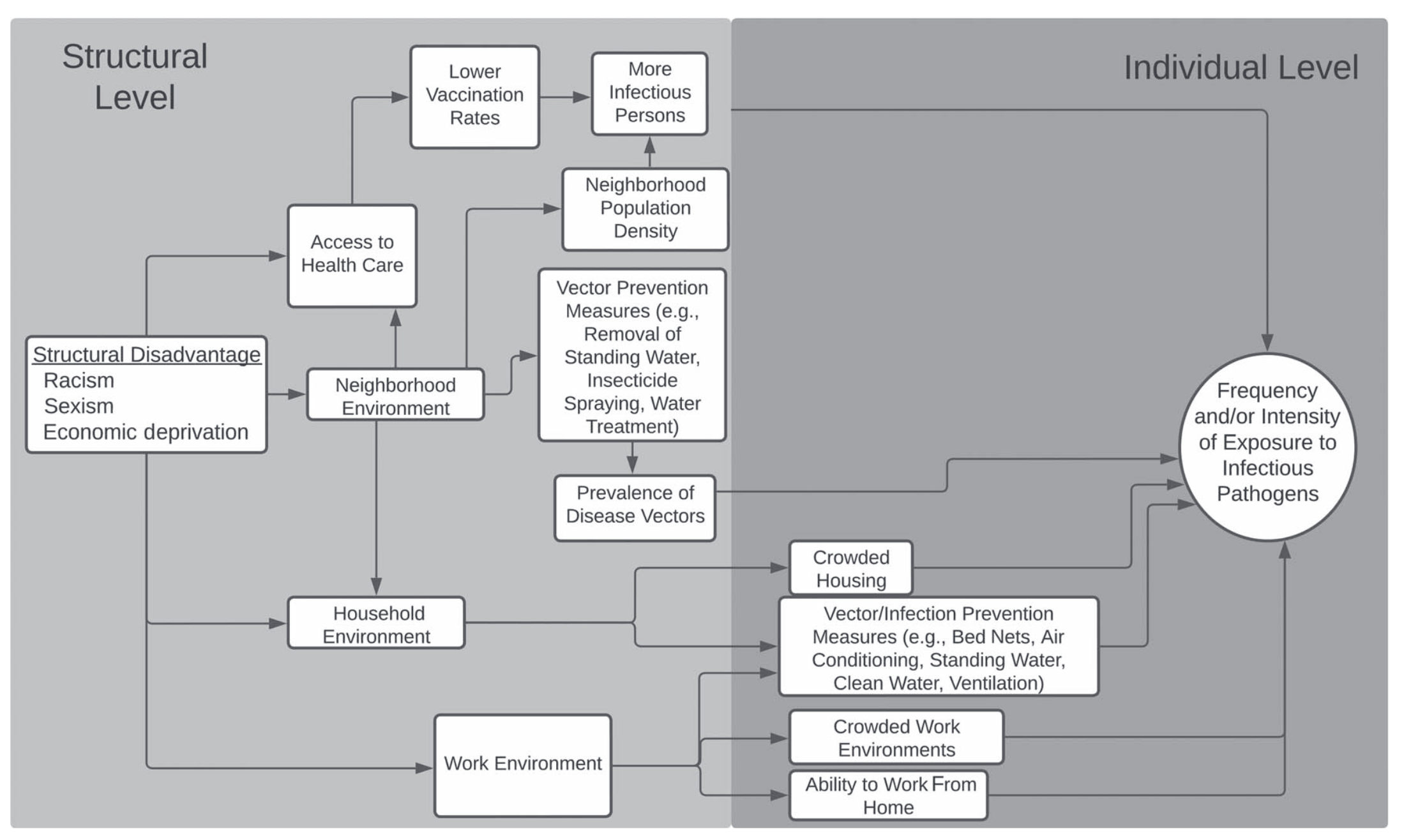
Flow diagram of connections between high-level, structural causes, intervening mechanisms, and downstream exposure risks, from (2)
Equity-oriented models cannot treat race and other social categorizations as causal variables.
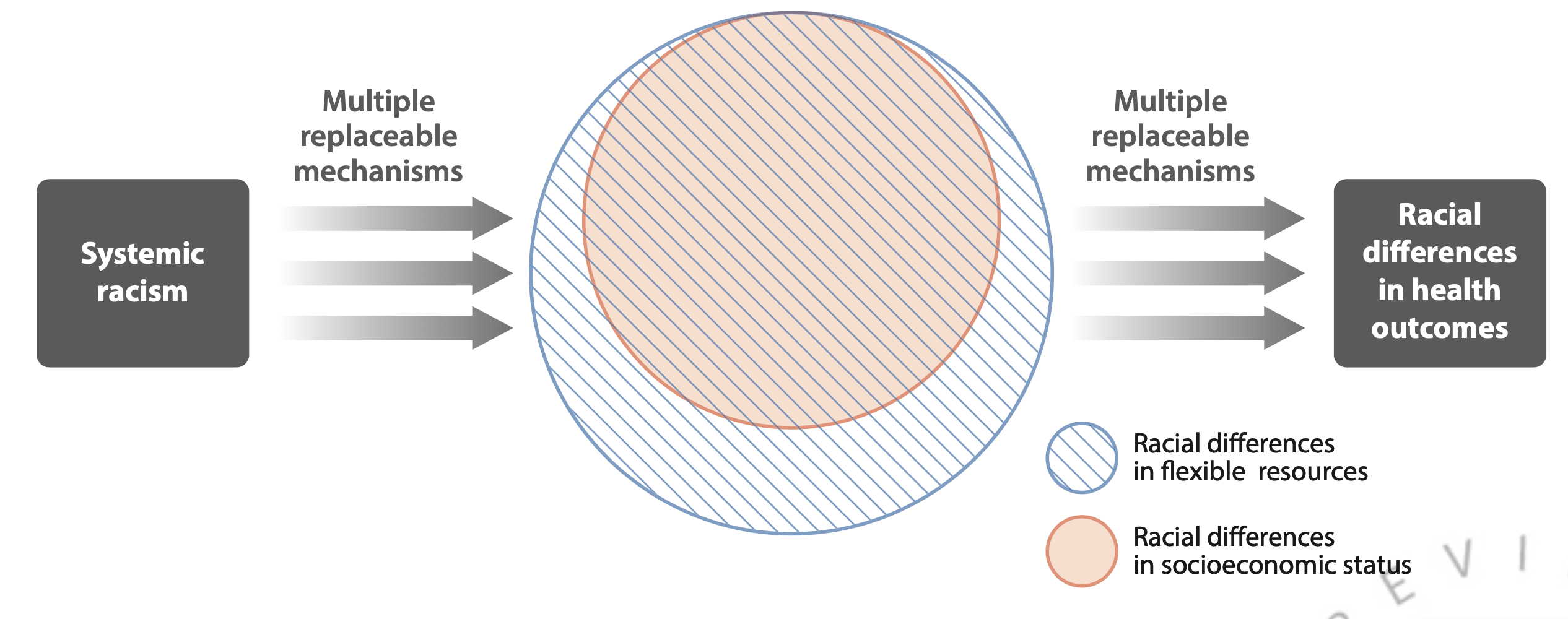
Theoretical diagram from (3) showing the complex relationship between racism, socioeconomic inequity and racial inequity in disease outcomes.
Equity-oriented models must use comparisons that reflect the impact of structural changes on disease risk.
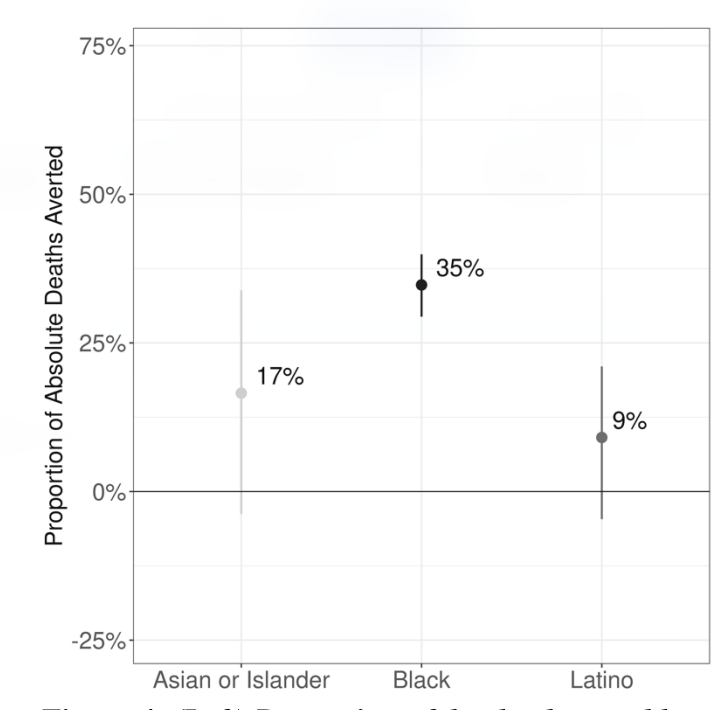
Proportion of SARS-CoV-2 deaths potentially averted in 2020 if all Michiganders experienced the same pacing of SARS-CoV-2 infection as Whites (From Naraharisetti et al., Under Review)