08:00
What does segregation do in infection processes?
EPID 684
Spatial Epidemiology
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
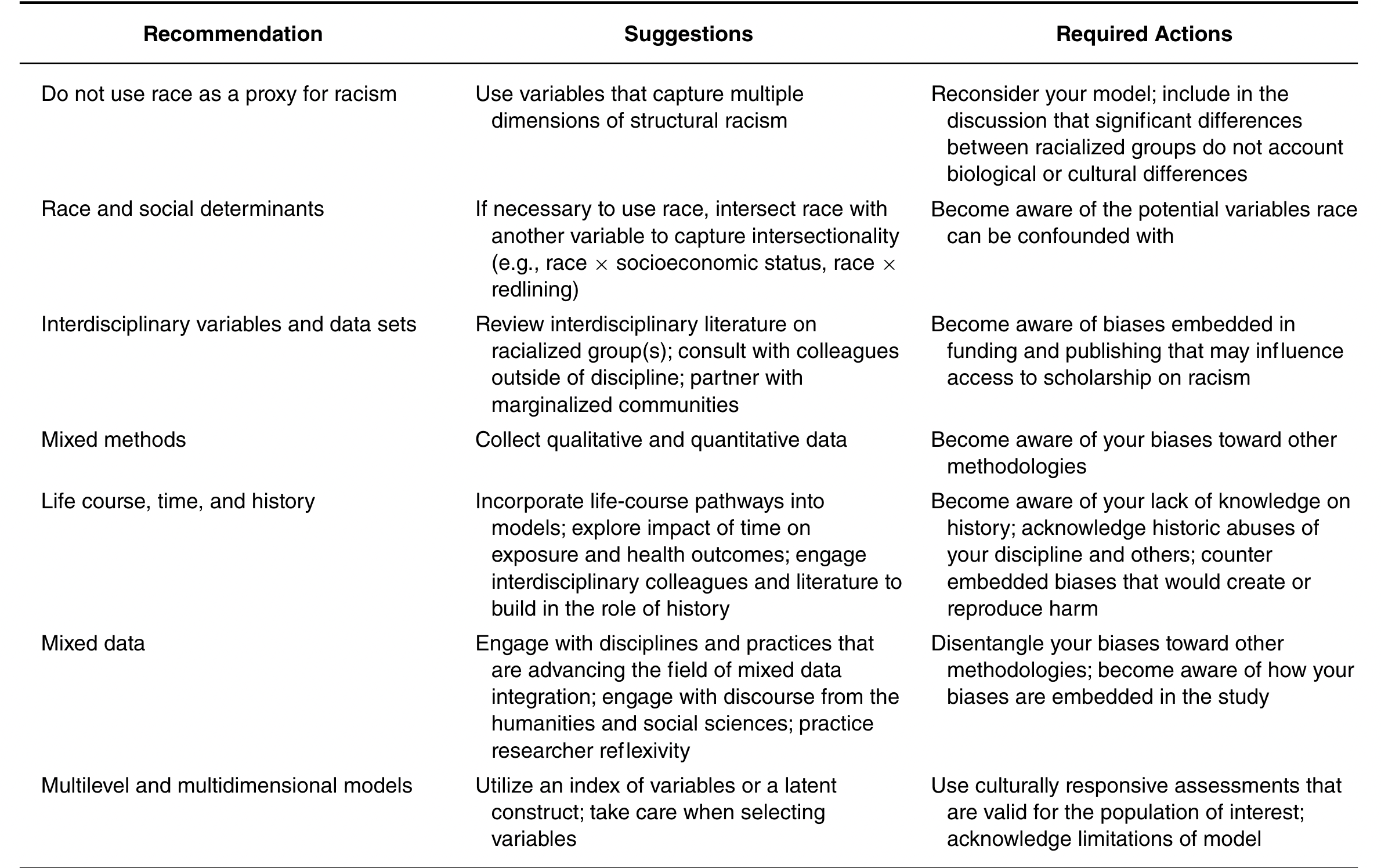
What are the challenges and risks of trying to account for structural racism in disease outcomes?
Economic and racial inequity is a central story of the COVID-19 pandemic





So why were we not prepared for these easy-to-foresee inequities?
The myth of the equal opportunity infector may have obscured inequality

OK, but this was so obvious!
How did we miss the fact that justice is a critical dimension of preparedness?
Historical analyses have repeatedly demonstrated inequity in prior pandemics
The mechanisms of inequity were quickly identified, but our models weren’t ready for them
What might an alternative framework look like?
- Model spatially localized infection risks as a function of upstream social determinants.
- Represent correlation between effects of factors such as racism and SES on spatial variation in infection risks.
- Examine differential impacts of social inequity on contact, susceptibility, and infectiousness.
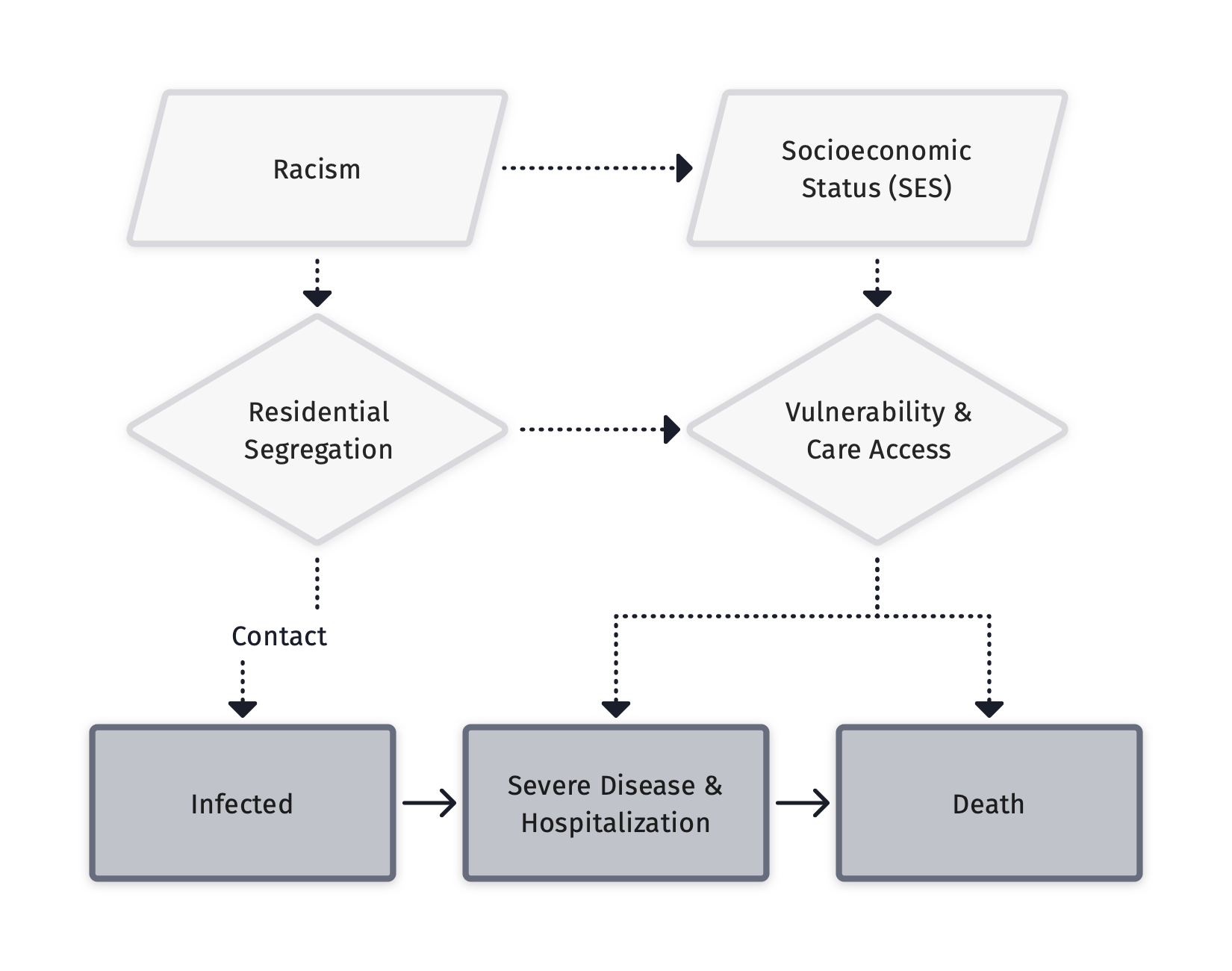
Zelner et al. (2022), There are no equal opportunity infectors. PLOS Computational Biology
This shift is already well underway
And it reflects recent experiences as well as ideas that have been bumping around for awhile
These equity-oriented models let us ask crucial questions about the causes of disparity
From Nande et al. “The effect of eviction moratoria on the transmission of SARS-CoV-2”, Nature Communications, 2021
OK: Here’s my stab at doing a better job of modeling the drivers of inequity in infection risks
Hands-on with a mechanistic version of this model