Causes, Fundamental
PUBHLTH 405
Social Epidemiology of Infectious Disease
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
Goal for Today
Getting ready to read Infectious Fear
“The purpose of a system is what it does.”
It’s easy to mistake the POSIWID view of the world for a slightly tiresome kind of cynicism. To say that the purpose of the system is what it does isn’t to make any statement about the intentions of the people working for it. The danger of confusing the properties of the system with those of its members is one of the most important reasons for not opening up a black box. Unfortunately, it’s a very common confusion; very few people are able to take a step back, view their own organisation as if from outside, and realise that they are structurally producing results which are exactly the opposite of what they had intended. (Davies 2024, 53)
Why is racism a fundamental cause on top of SES?
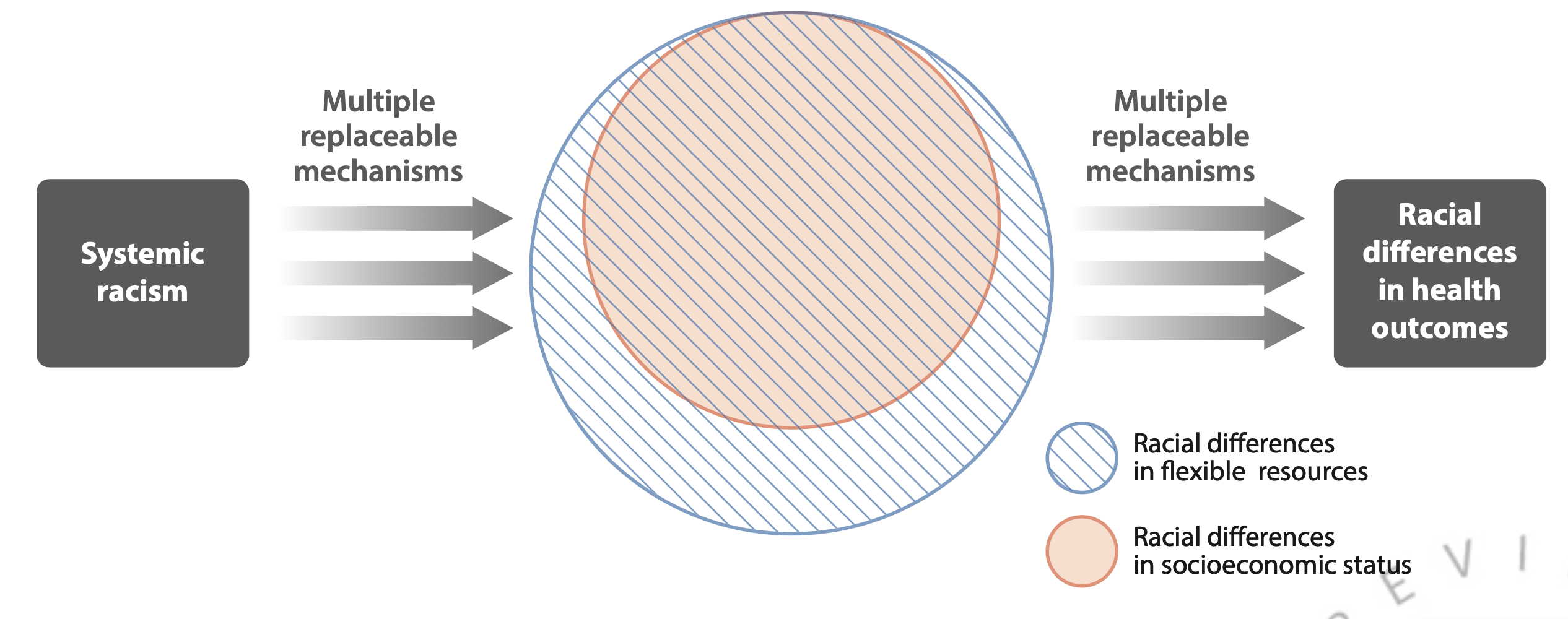
Why can’t socioeconomic status explain all race/ethnic health inequities?
Residential segregation may compound impacts of SES and racism.
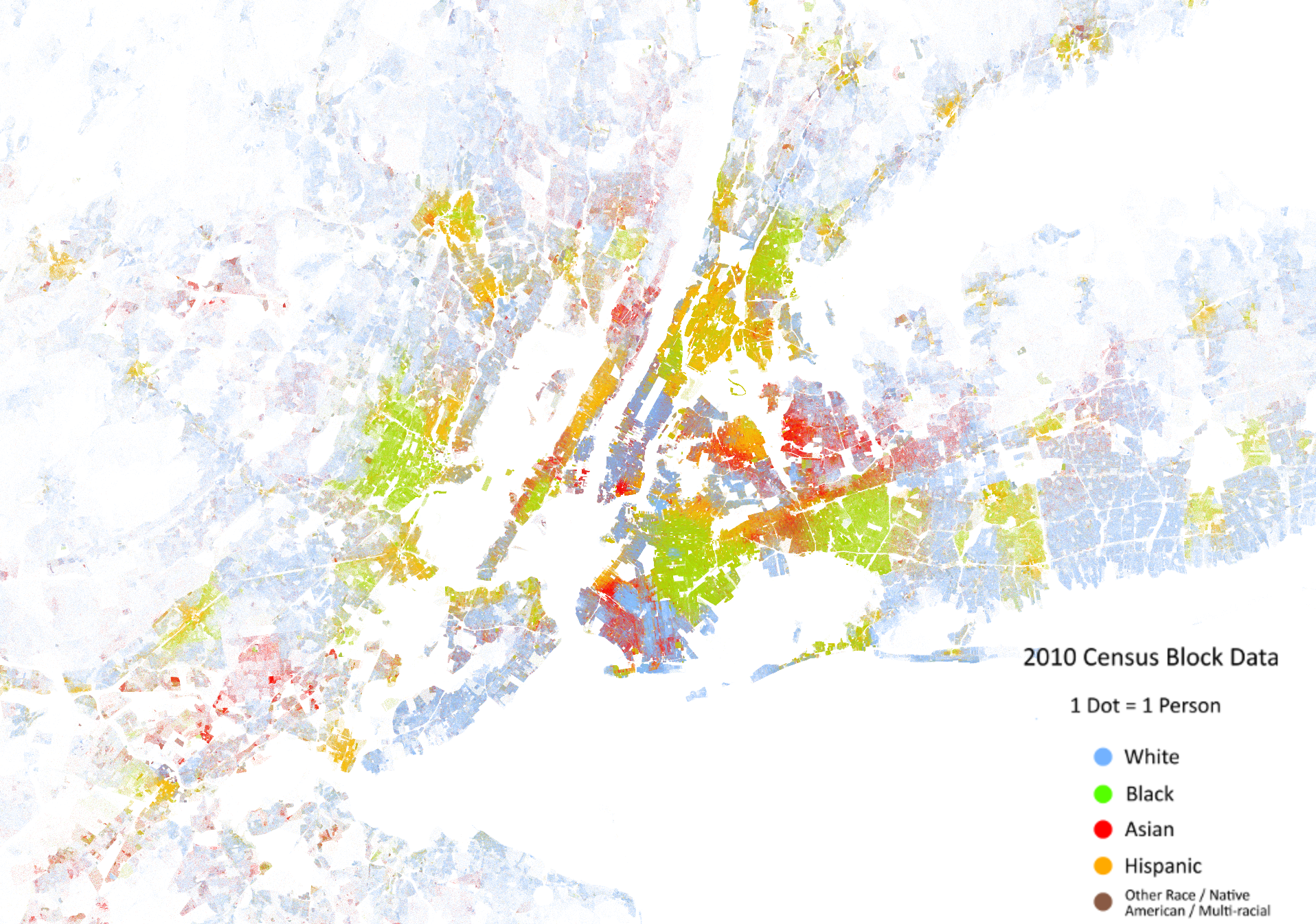
What intervening mechanisms are we talking about when we talk about segregation as a fundamental cause? (map from (ESRI 2022))
This leads to a relatively predictable life-cycle of inequity
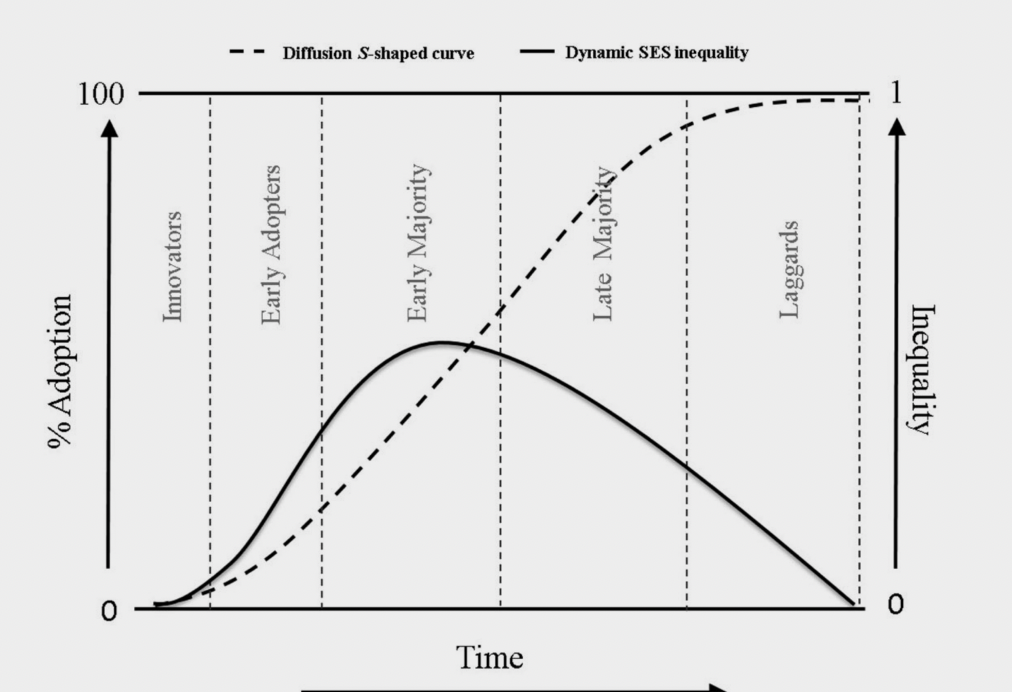
Example of how inequity rises and falls as an innovation diffuses through the population from (Zapata-Moya, Willems, and Bracke 2019)
We can see the generation of inequality during the first phases of covid
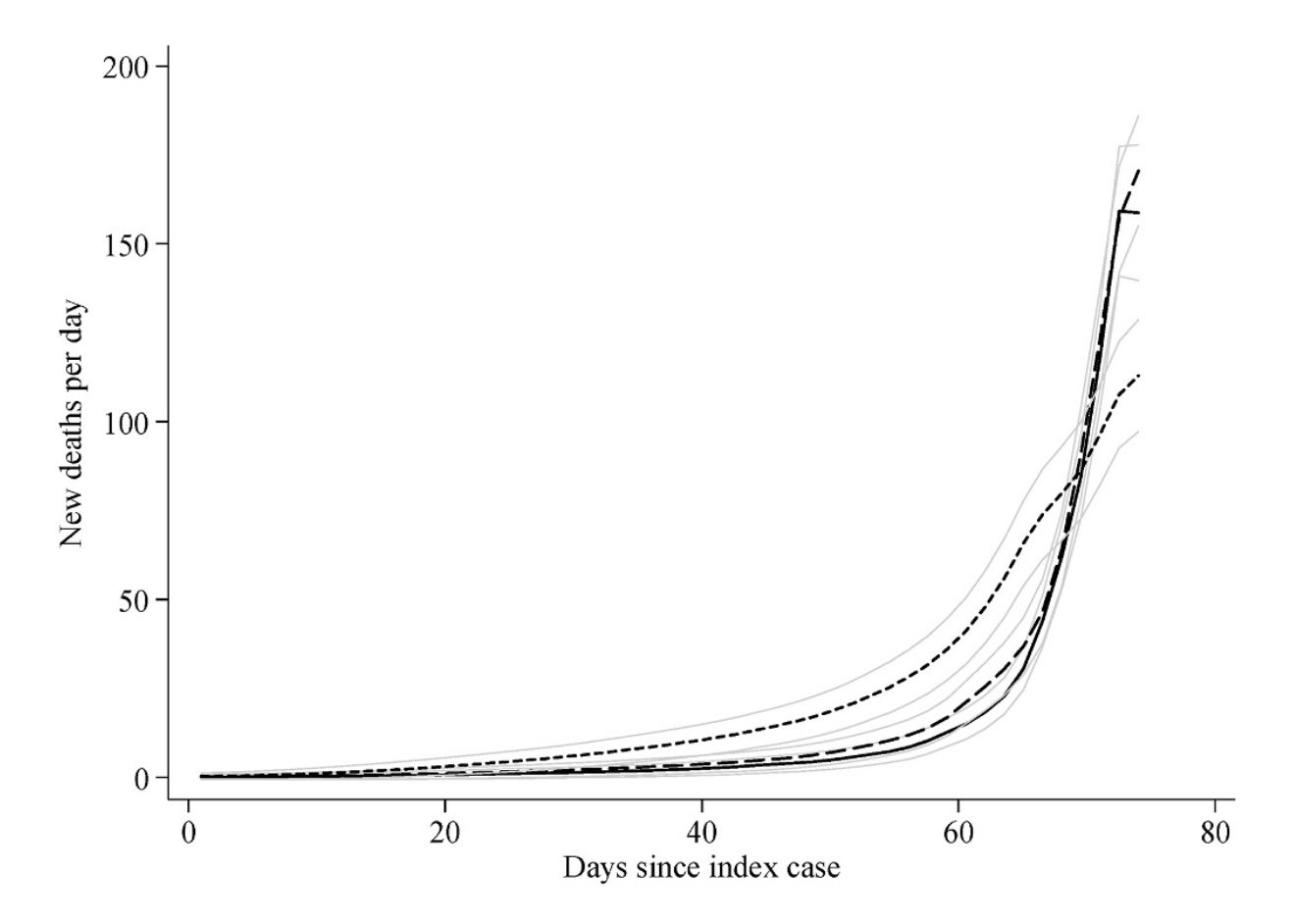
Changes in SARS-CoV-2 mortality by SES of U.S. counties. High SES counties are represented by the short-dashes, all others by long-dash and solid line (from (Clouston, Natale, and Link 2021))
What interventions or policies might explain this pattern?
Socio-structural inequities drive unequal outcomes across the entire life-cycle of infection
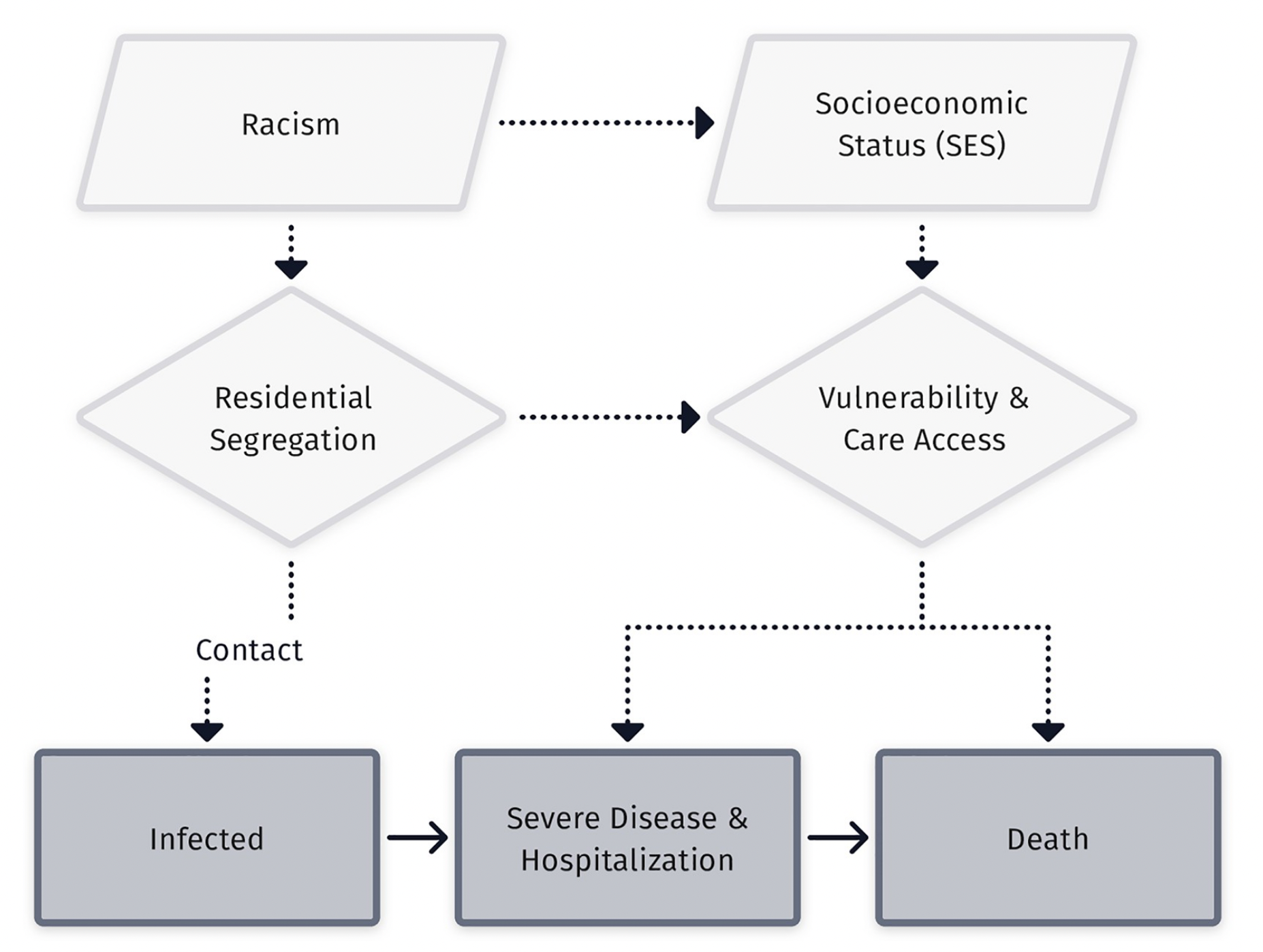
Flow diagram from Zelner et al. (2022)
What is the distinction between inequity in exposure versus susceptibility?
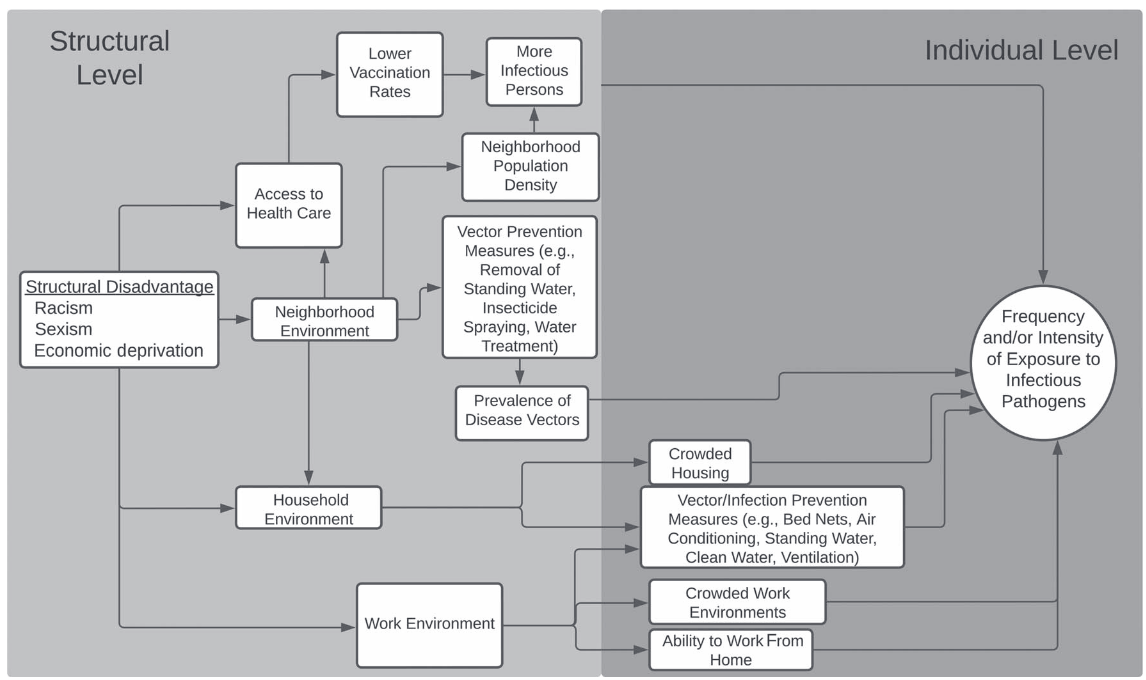
Mechanisms leading to differential exposure to infection from (Noppert, Hegde, and Kubale 2022)
What is the distinction between inequity in exposure versus susceptibility?
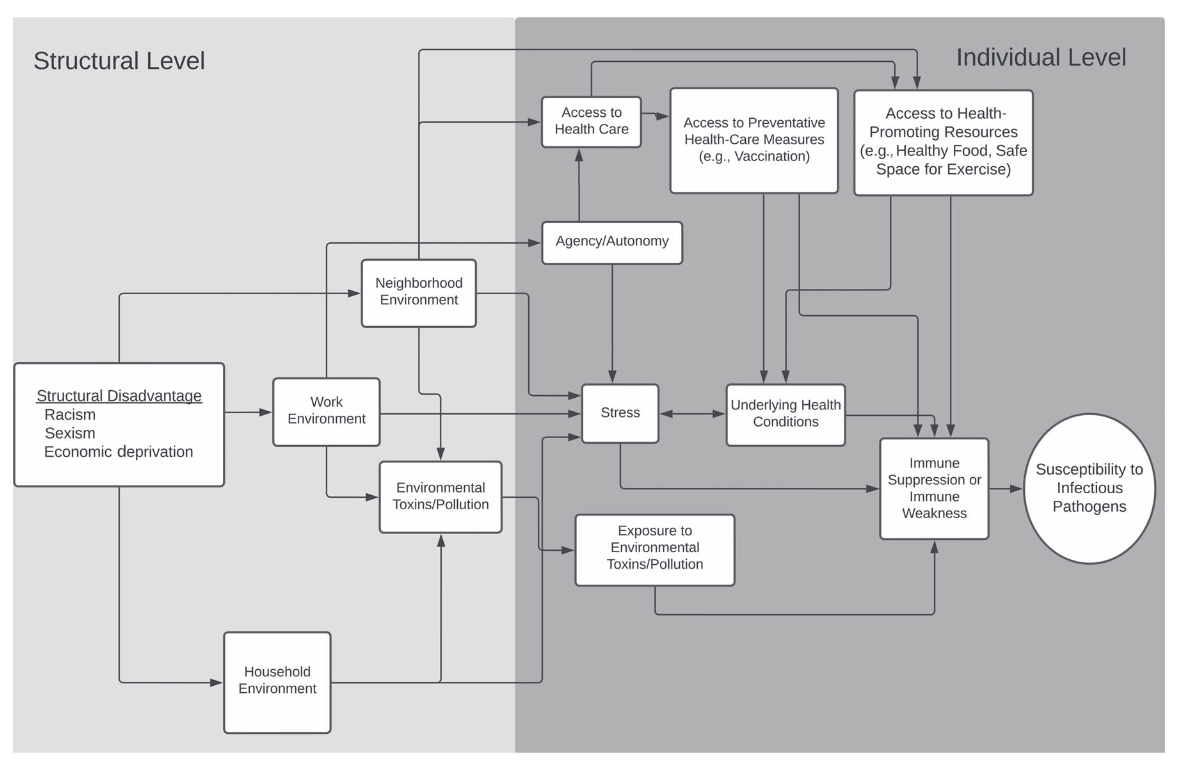
Mechanisms leading to differential vulnerability to infection from (Noppert, Hegde, and Kubale 2022)
Link & Phelan identified structural determinants of infection inequity in their original work
An example of how fundamental causes may be reflected in foodborne infection (Link and Phelan 1995)
Next Time
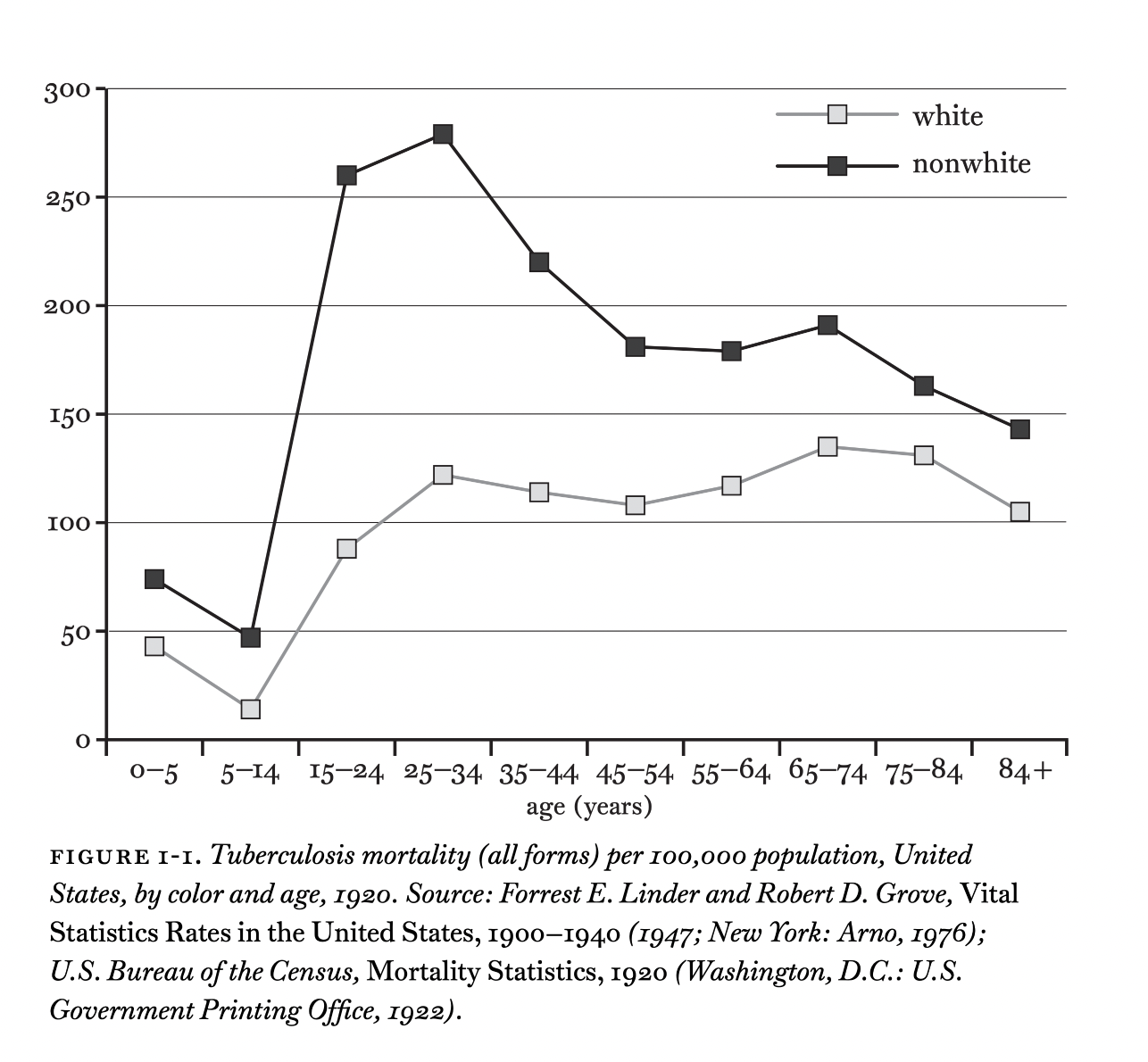
Racial inequality in Tuberculosis infection and mortality in the 20th Century