05:00
Tuberculosis as a reflection of inequality
PUBHLTH 405
Social Epidemiology of Infectious Disease
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
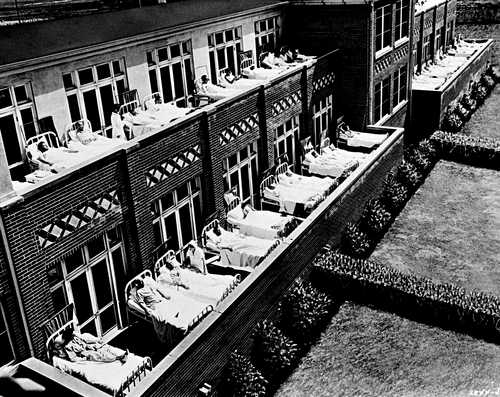
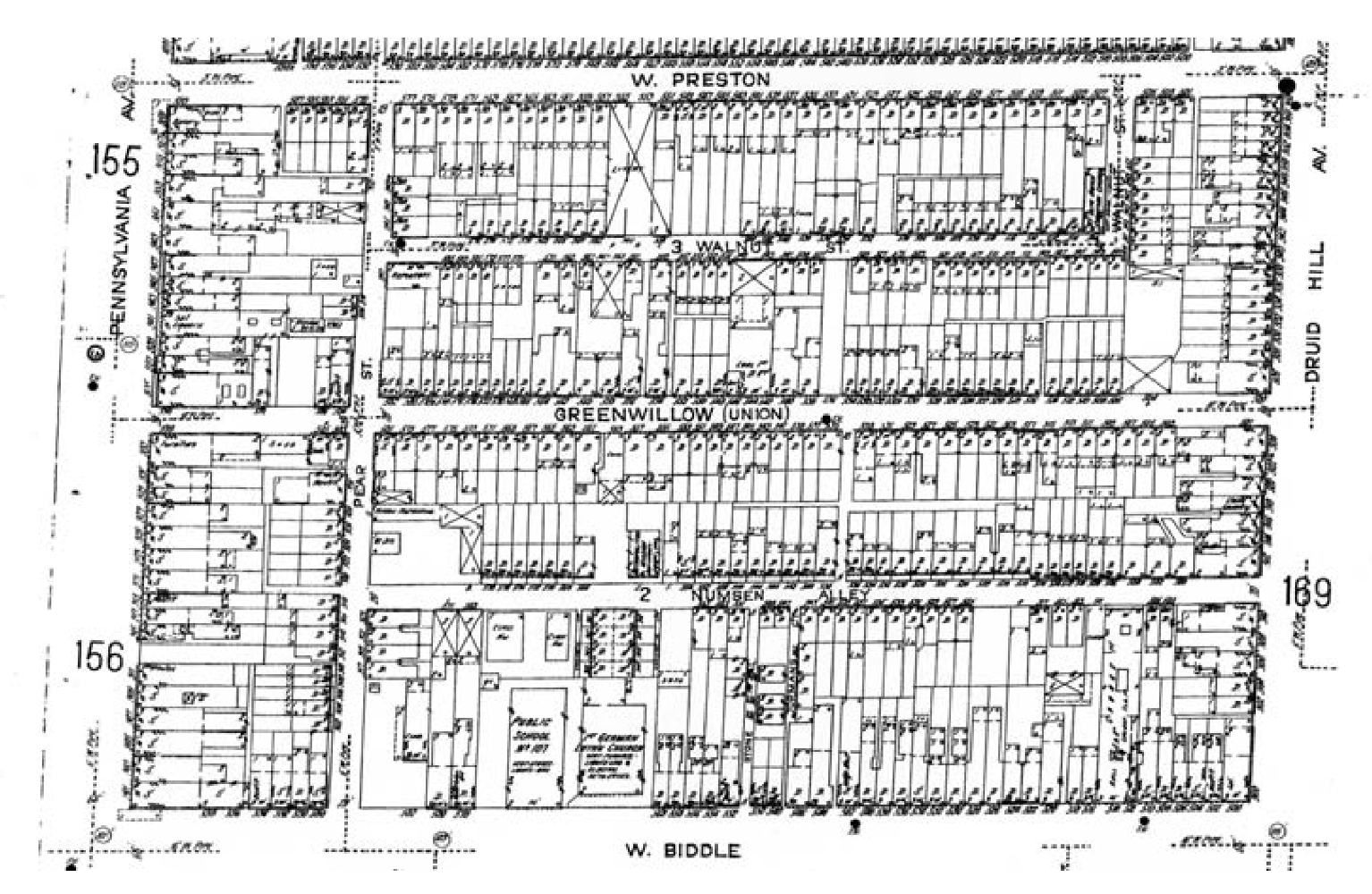
What were TB Sanitoria?

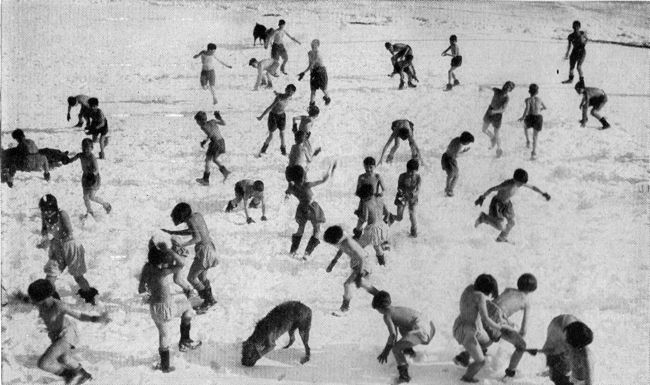
Respiratory infection with transmission facilitated by close contact
Anti-TB poster from the American Lung Association
TB can become latent or dormant in the body and re-emerge
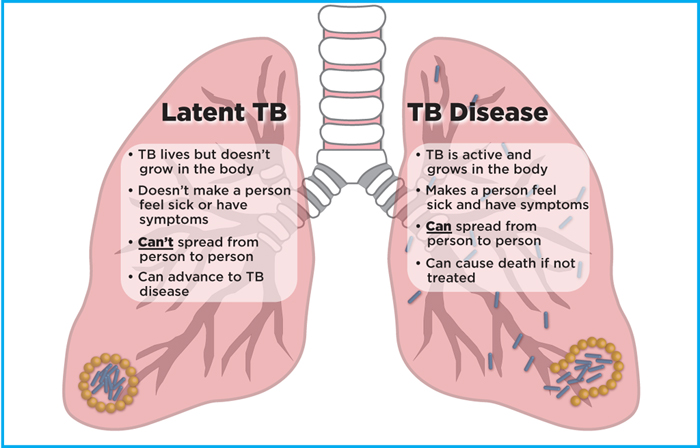

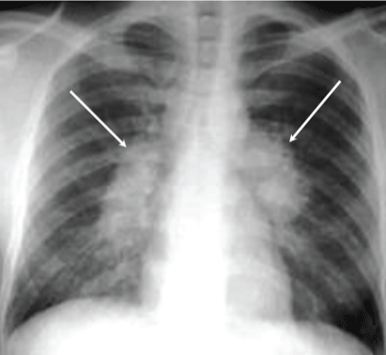
TB Diagnosis
Active TB
Latent TB
What do these different measures tell us about burden in the population?
In the U.S., TB declined dramatically over the course of the 20th century
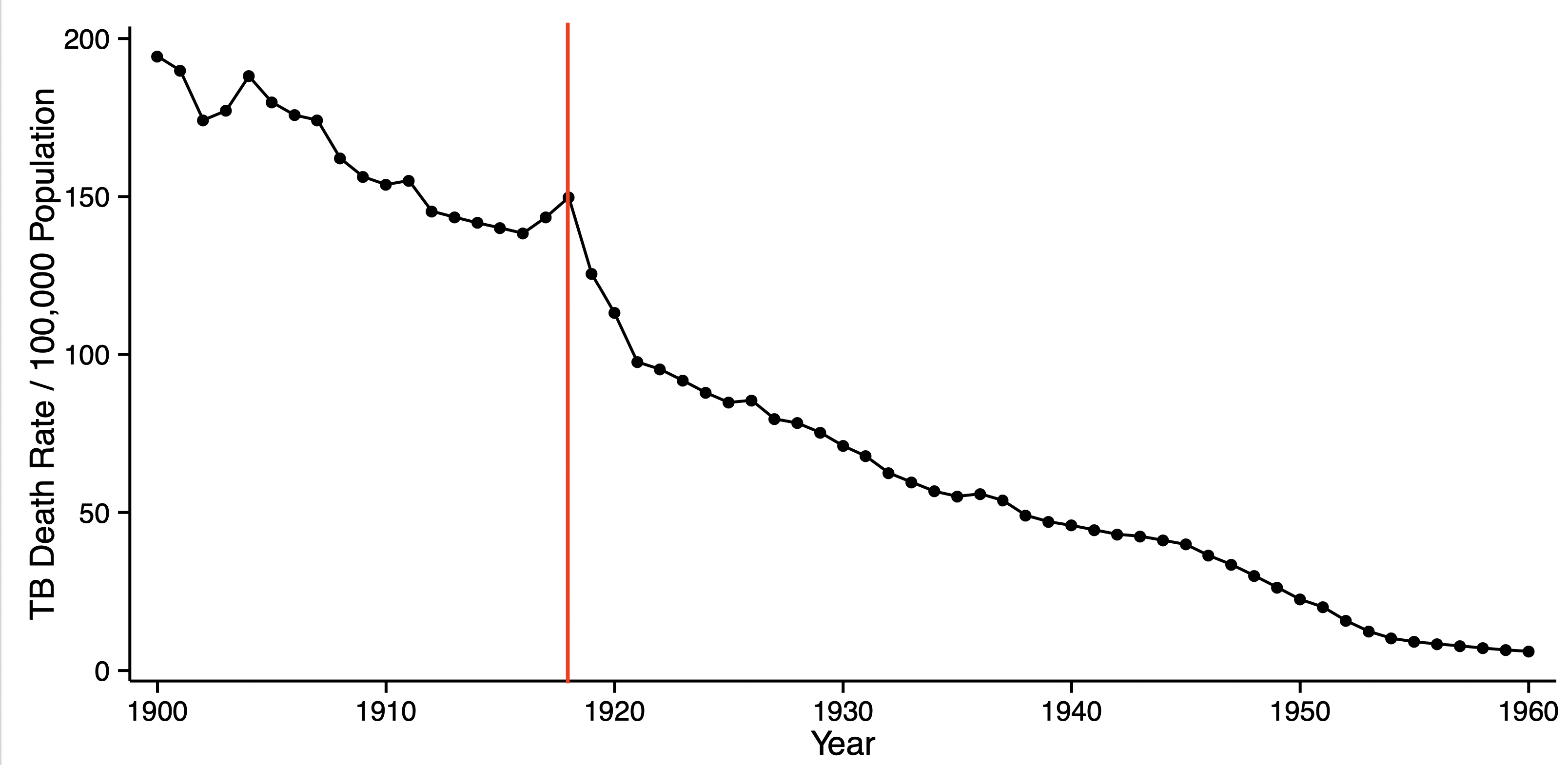
What happened at the time where the red line is?
But: Availability of effective TB treatments followed these declines

A brief history of TB science and treatment
Present-day TB incidence is highest in Sub-Saharan Africa
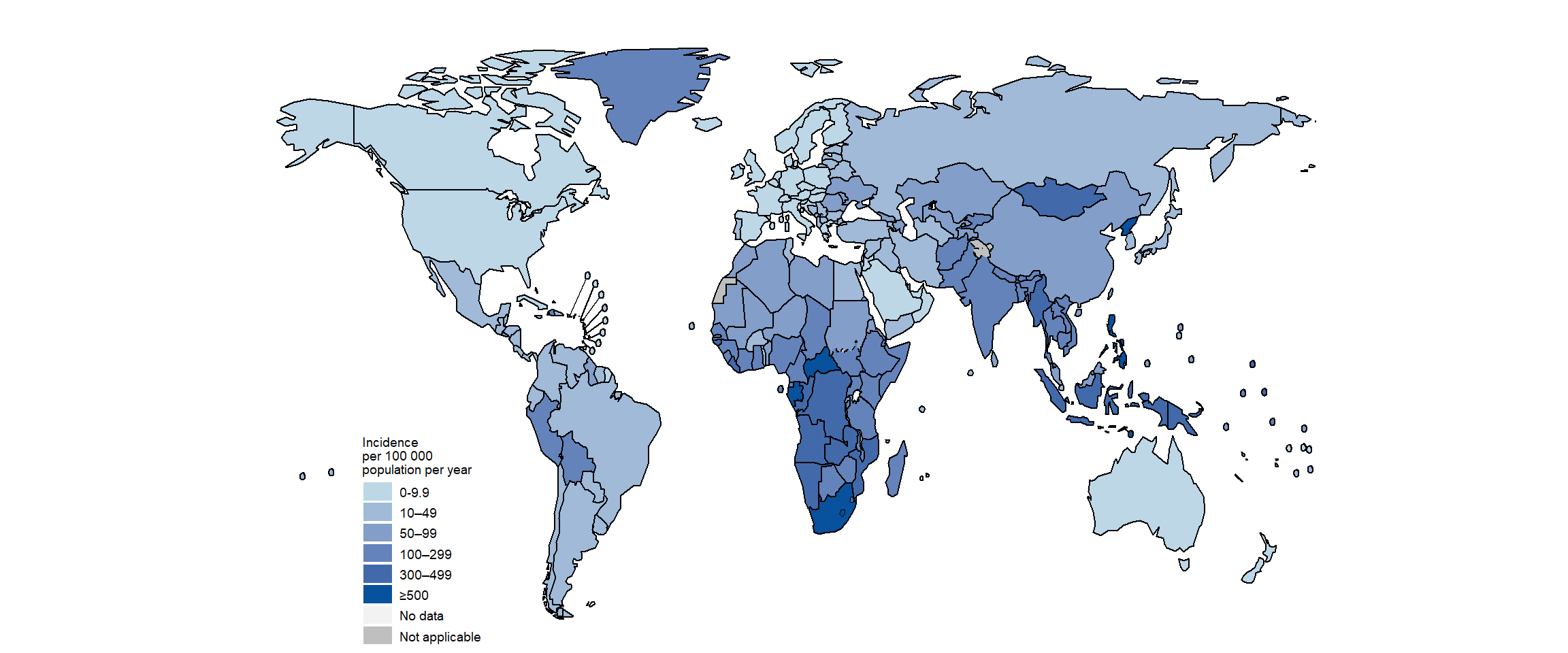
Global TB incidence from the 2021 WHO Global TB Report
TB incidence and mortality is now strongly correlated with HIV prevalence
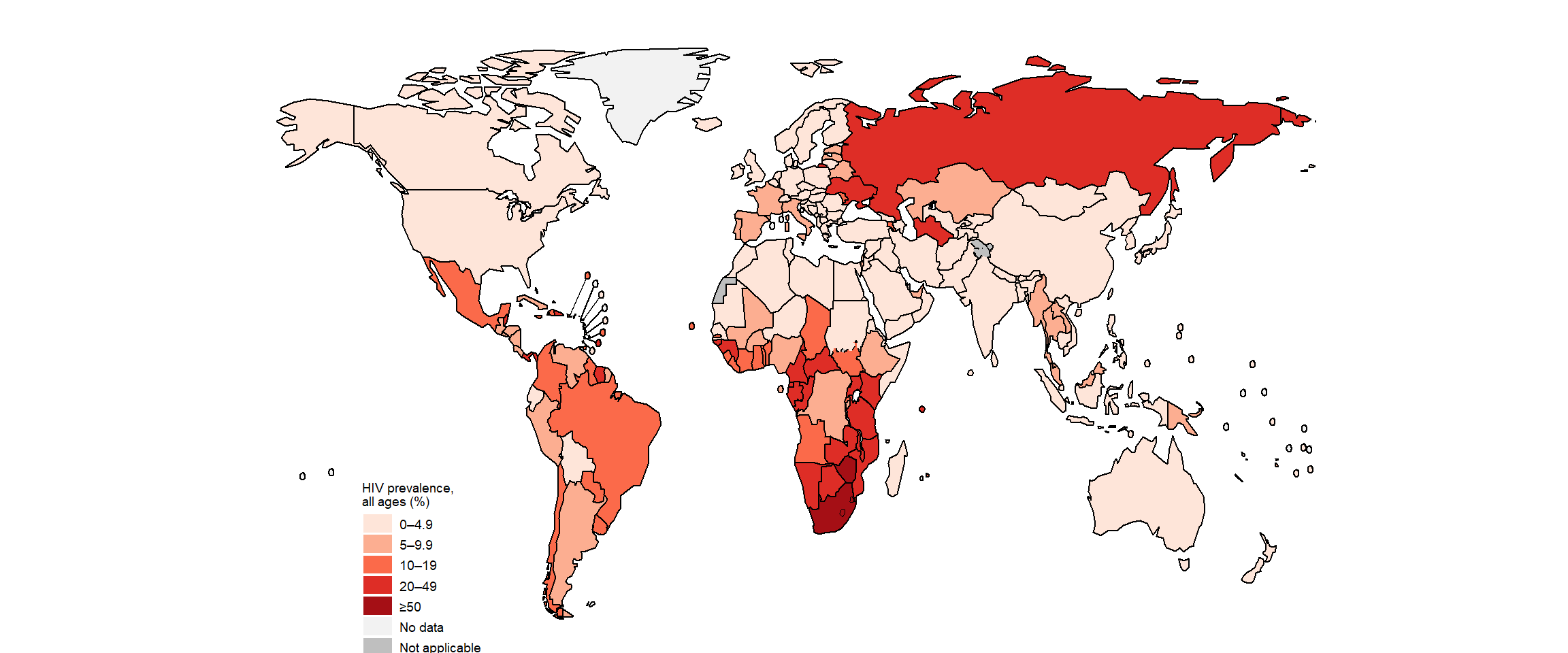
Proportion of new and relapse TB cases that are HIV+ in 2020
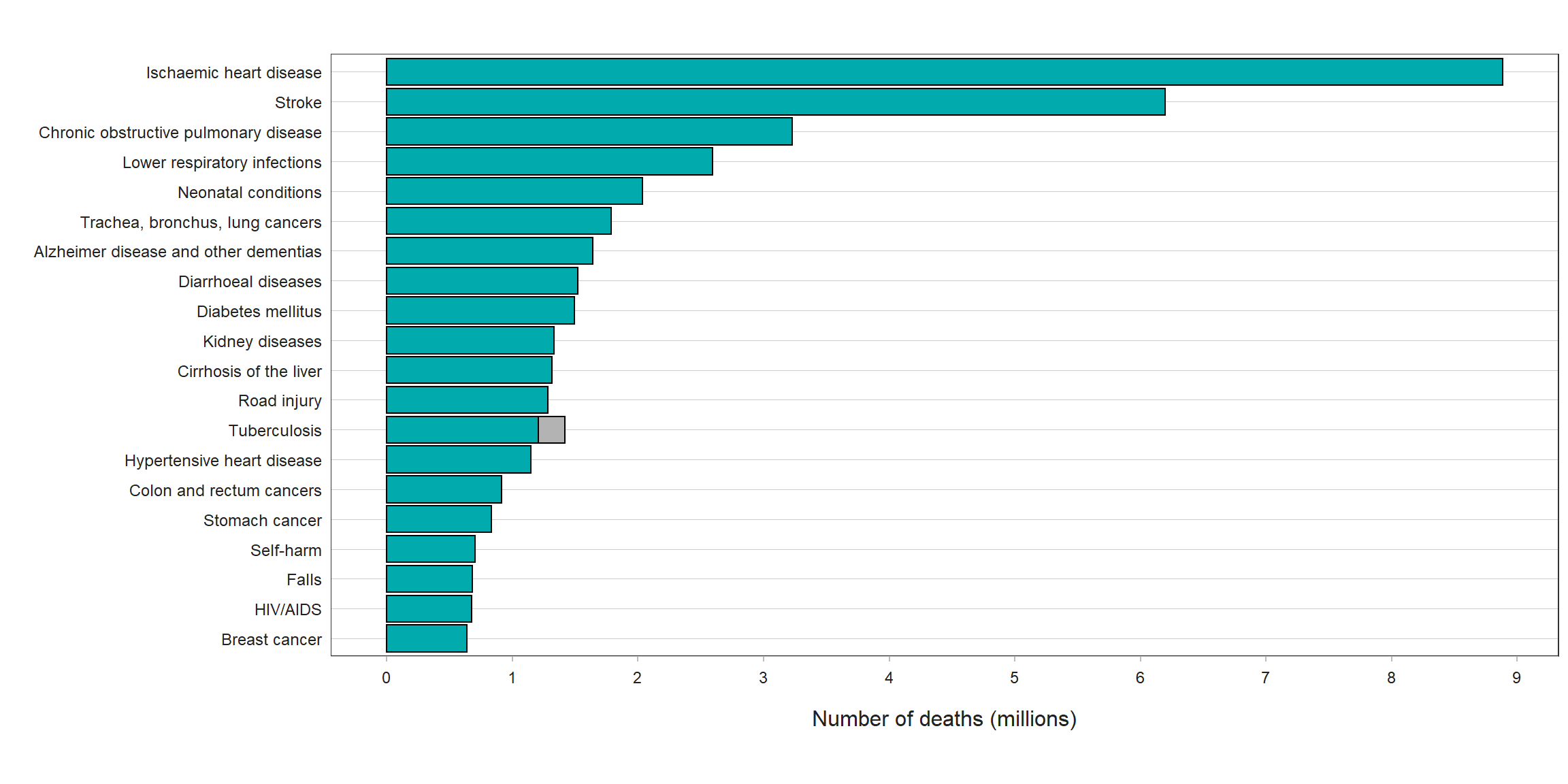
TB is the most common cause of death from infectious disease worldwide
And: It is likely that COVID-19 has slowed or reversed the decline of TB in the U.S.
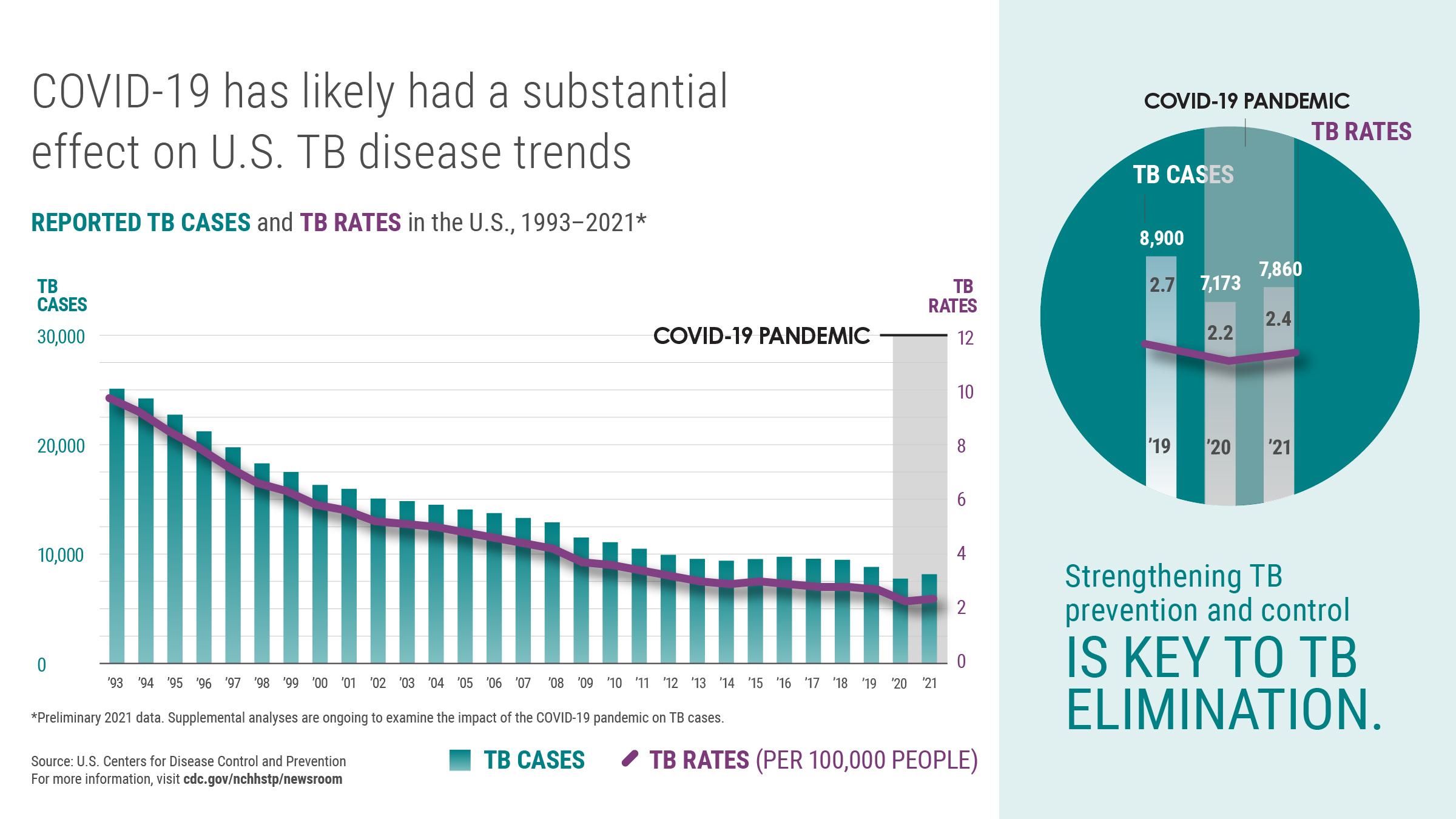
What are the likely implications of this backsliding for health equity? (Image from CDC)
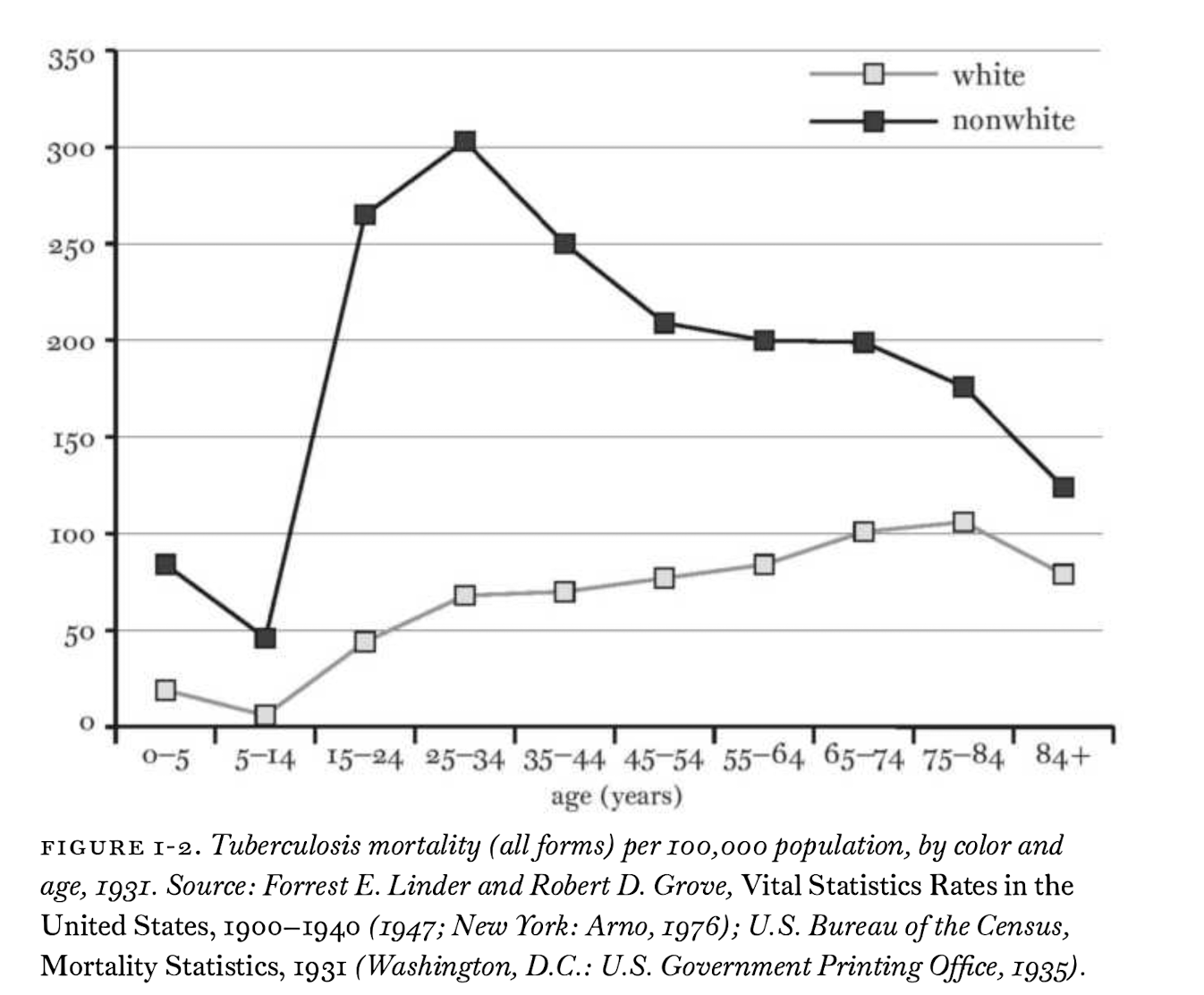
Patterns of infection and death by age tell us a lot about TB transmission
This leads to a relatively predictable life-cycle of inequity
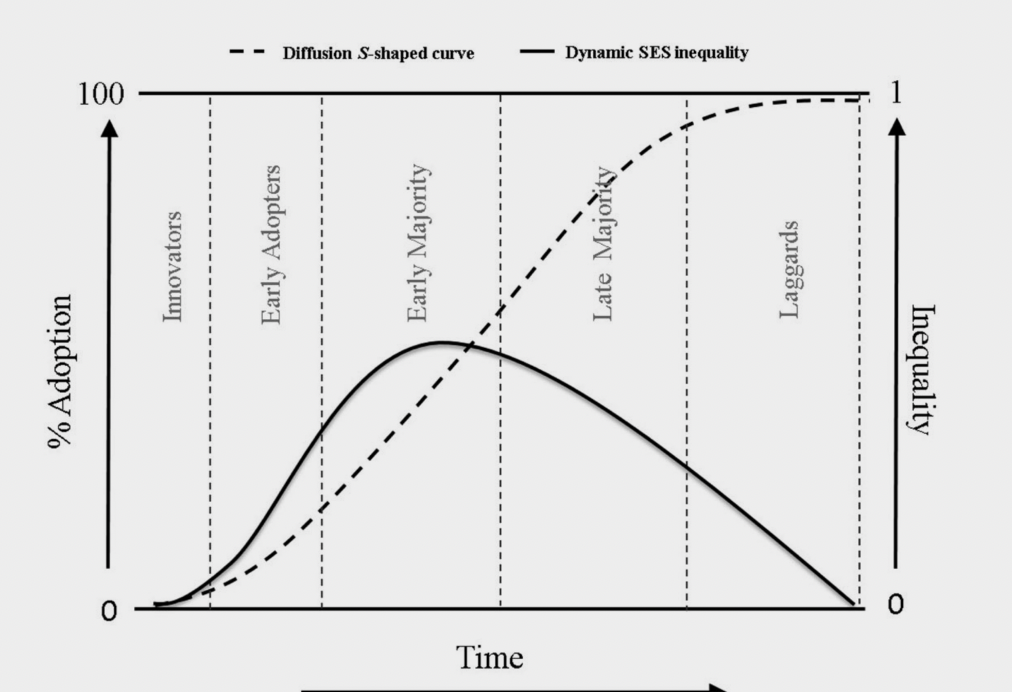
Example of how inequity rises and falls as an innovation diffuses through the population from (Zapata-Moya, Willems, and Bracke 2019)
We can see the generation of inequality during the first phases of covid
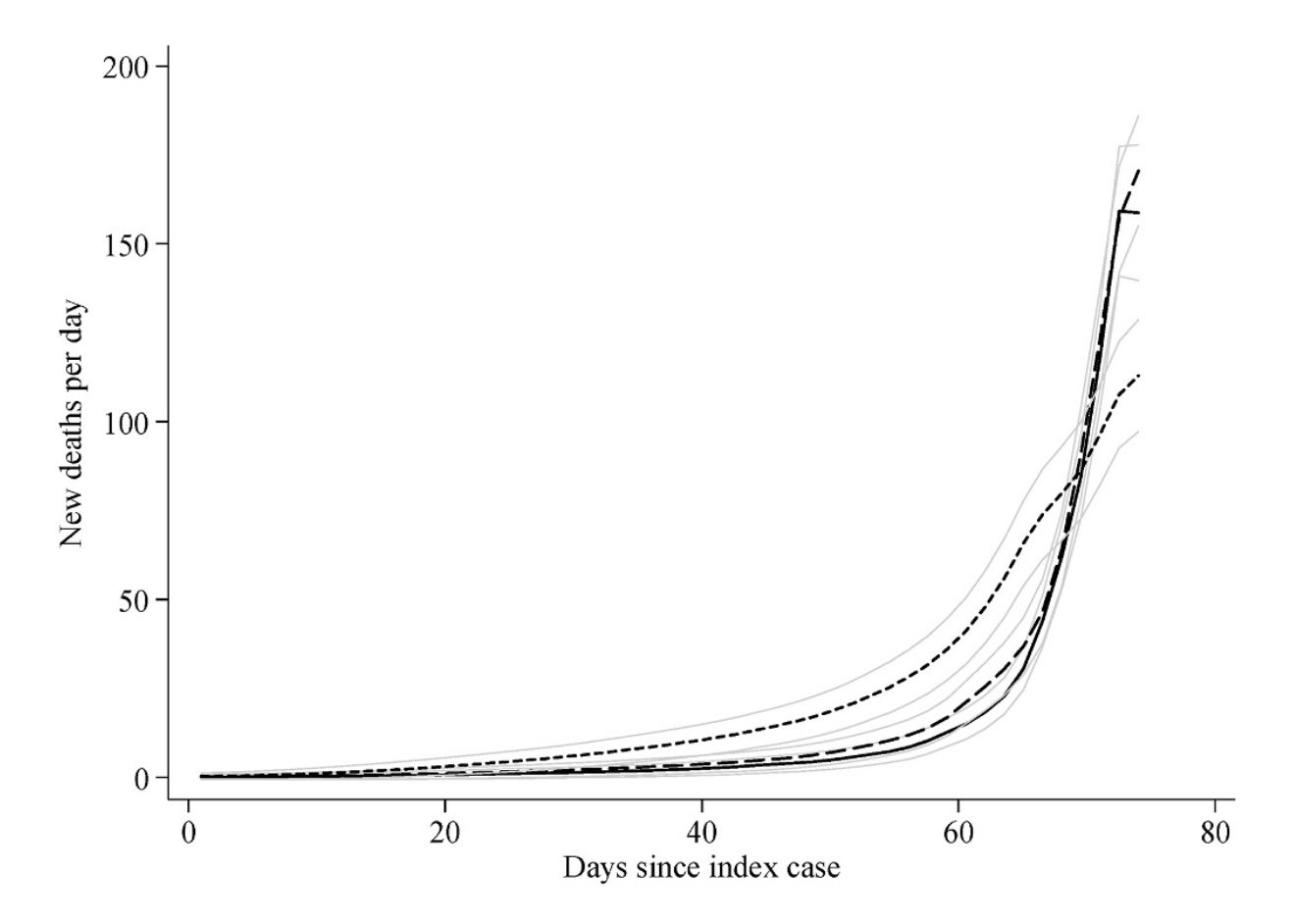
Changes in SARS-CoV-2 mortality by SES of U.S. counties. High SES counties are represented by the short-dashes, all others by long-dash and solid line (from (Clouston, Natale, and Link 2021))
What interventions or policies might explain this pattern?
Next Time
Chs 3 & 4: Connecting residential segregation to infectious disease transmission.
Important to remember: Segregation is not unique to the U.S. and only a reflection of racism
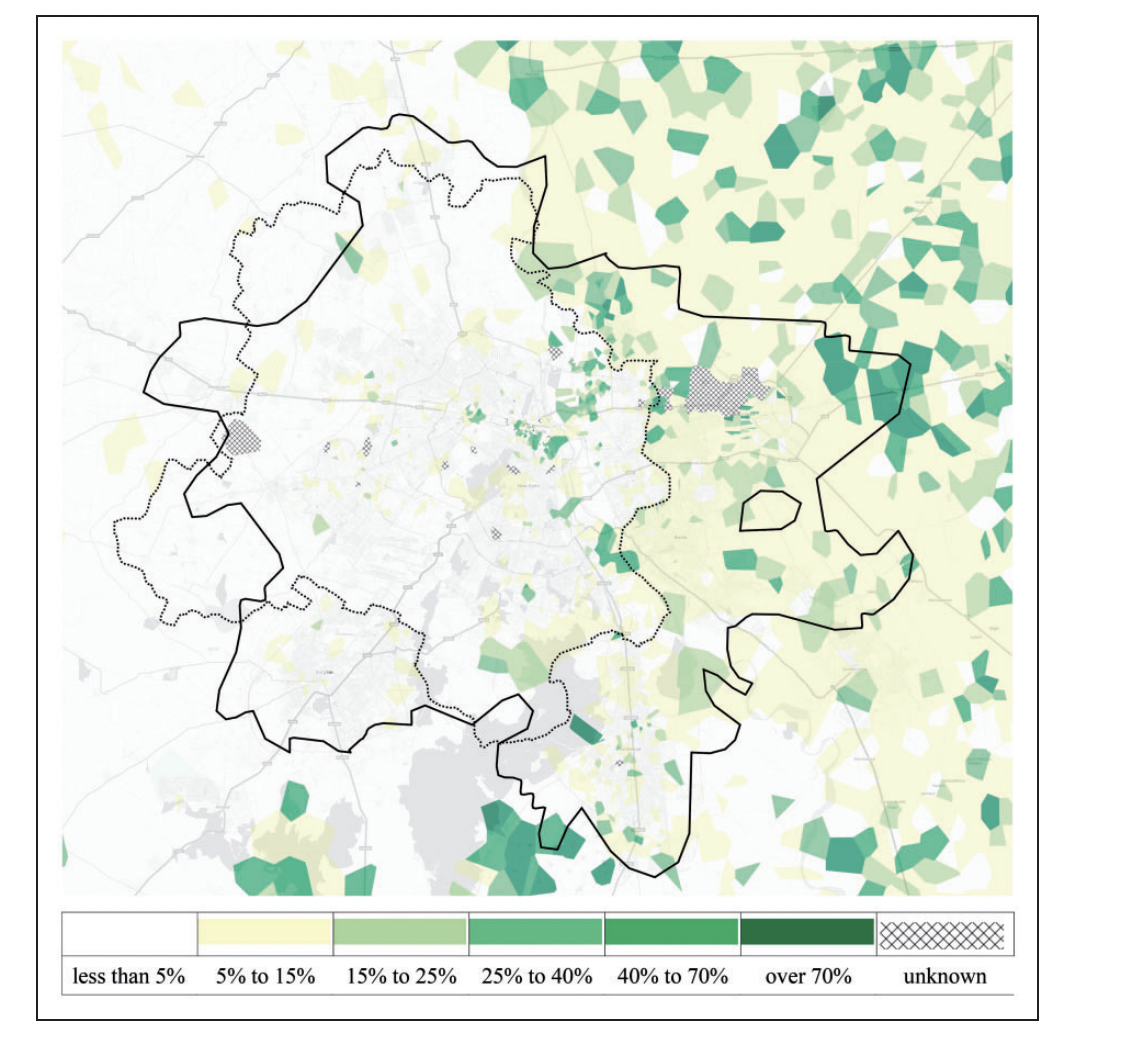
Residential segregation of Muslims and Hindus in Delhi, India (from (Susewind 2017))
Socio-structural inequities drive unequal outcomes across the entire life-cycle of infection
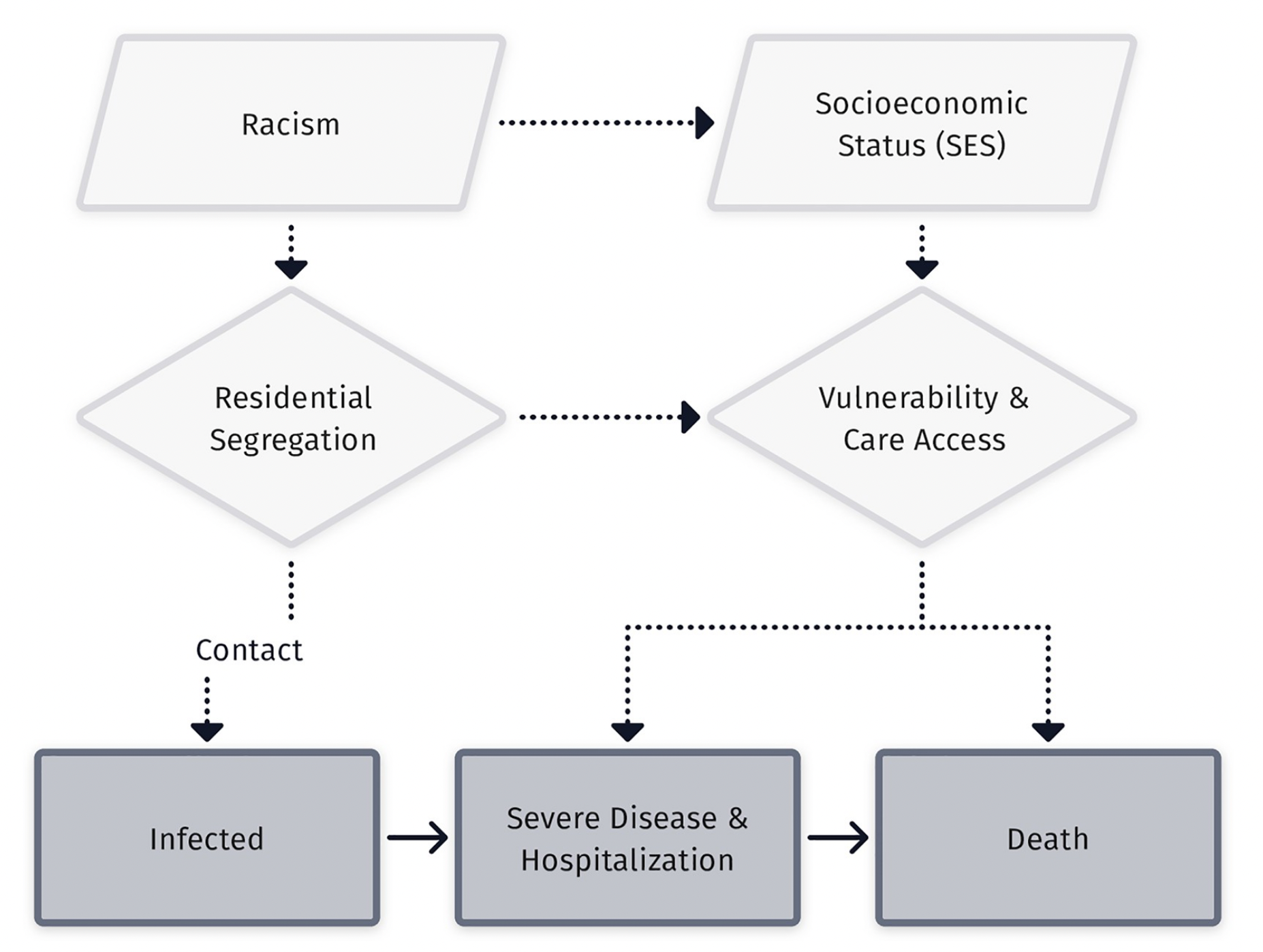
Flow diagram from Zelner et al. (2022)
What is the distinction between inequity in exposure versus susceptibility?
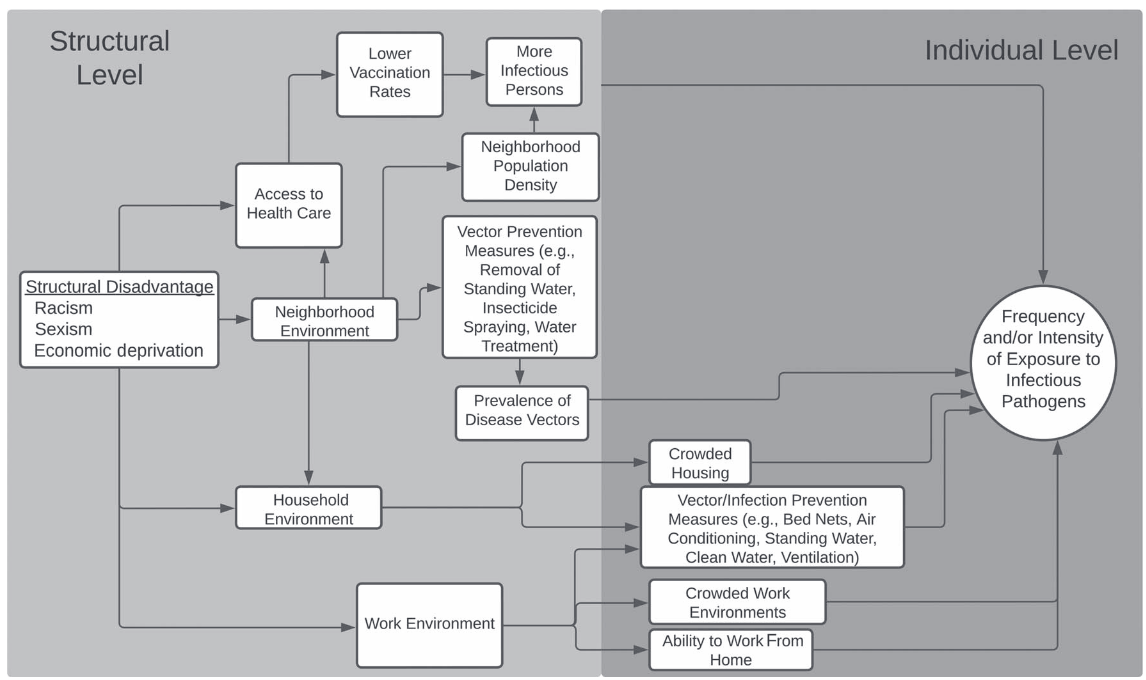
Mechanisms leading to differential exposure to infection from (Noppert, Hegde, and Kubale 2022)
What is the distinction between inequity in exposure versus susceptibility?
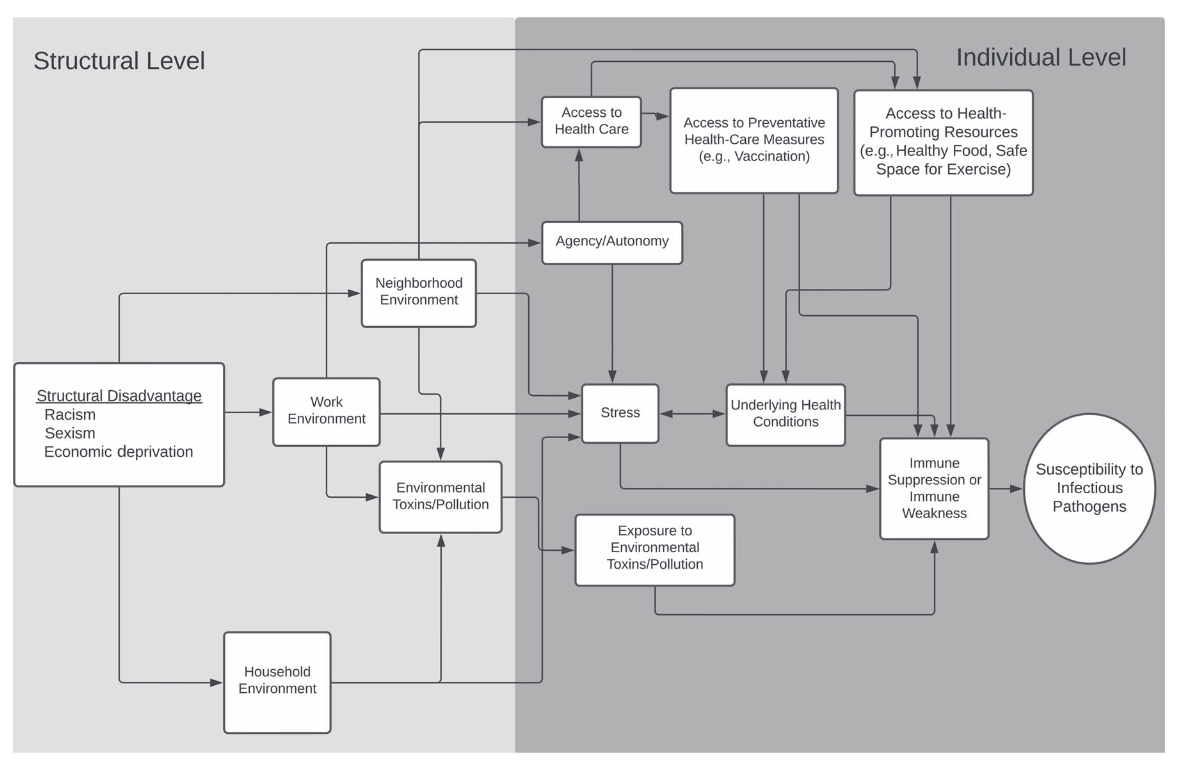
Mechanisms leading to differential vulnerability to infection from (Noppert, Hegde, and Kubale 2022)
Link & Phelan identified structural determinants of infection inequity in their original work
An example of how fundamental causes may be reflected in foodborne infection (Link and Phelan 1995)