05:00
Looking out at the Landscape of Health
PUBHLTH 405
Social History of Infectious Disease
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
Predisposition is the handmaiden of scientific racism in public health
“Particularly with regard to consumption it must be remembered that Negroes are not the first people who have been claimed as its peculiar victims; the Irish were once thought to be doomed by that disease - but that was when Irishmen were unpopular.” -W.E.B. Du Bois, The Philadelphia Negro, 1899
Alley houses in Baltimore reflected a unique mode of segregation
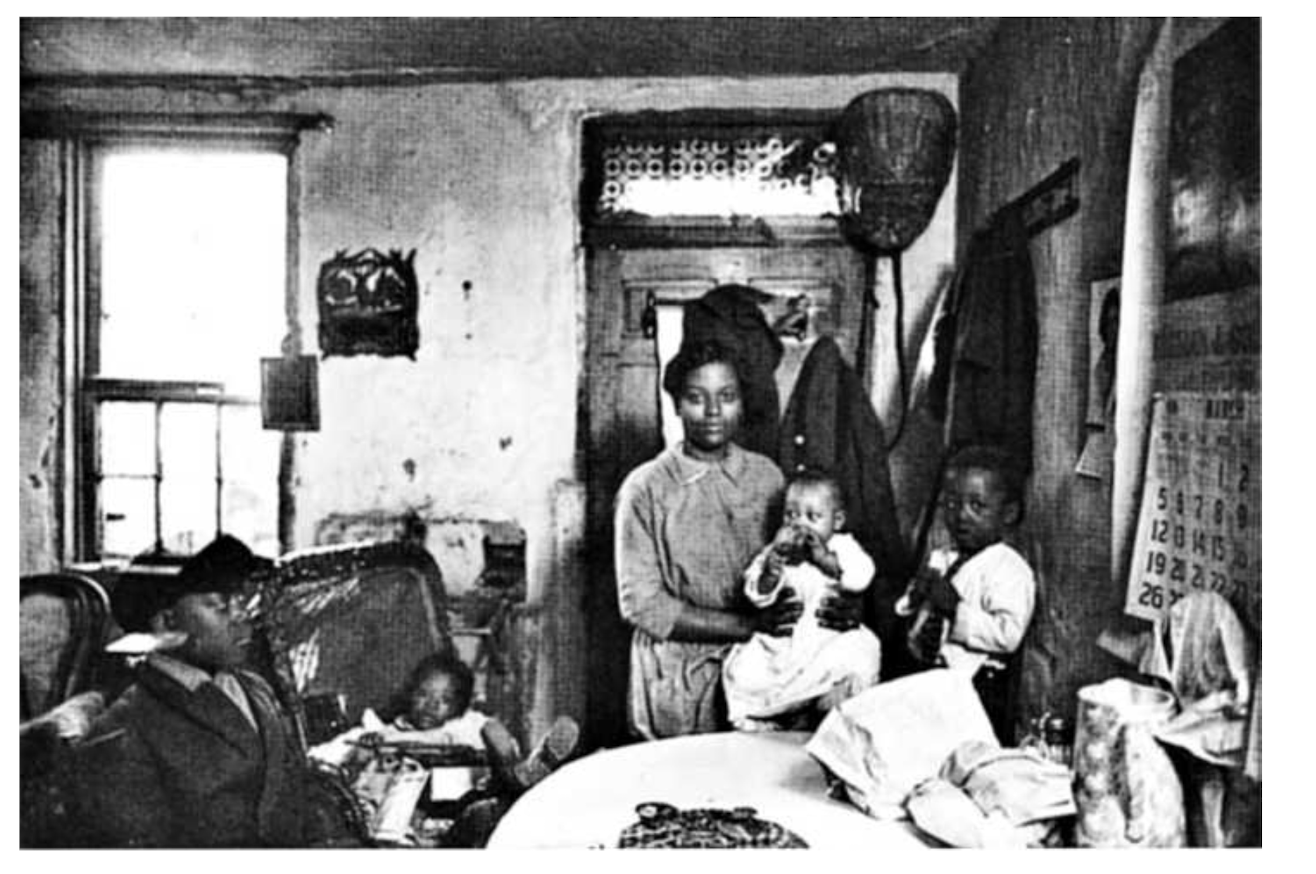
“In the lower-rent alleys between these two avenues could be found poorer blacks, who resided in one- or two-story houses whose front steps in many cases were separated from the opposite house by no more than six or eight feet of cobblestone or dirt.” (Roberts 2009)
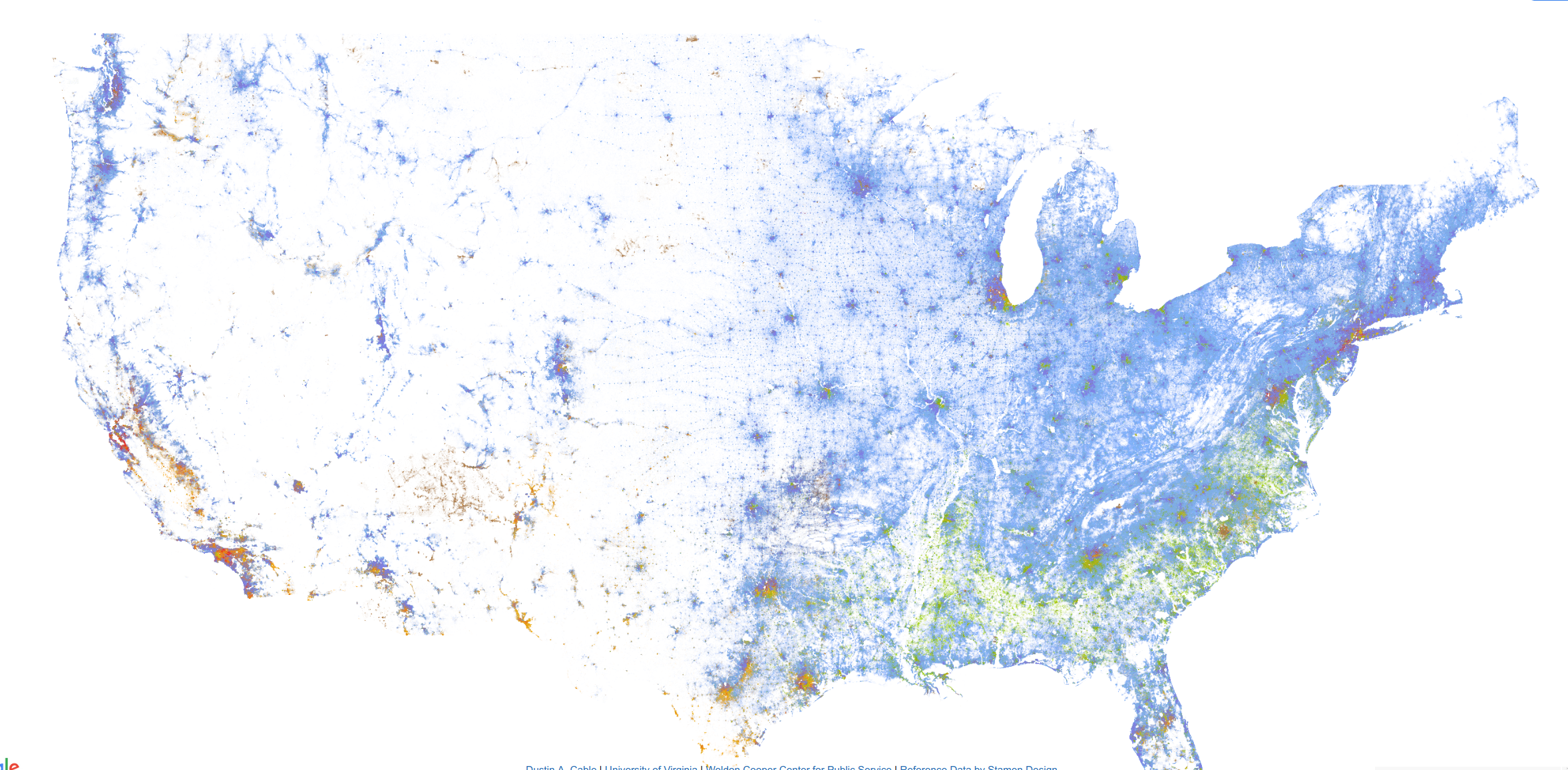
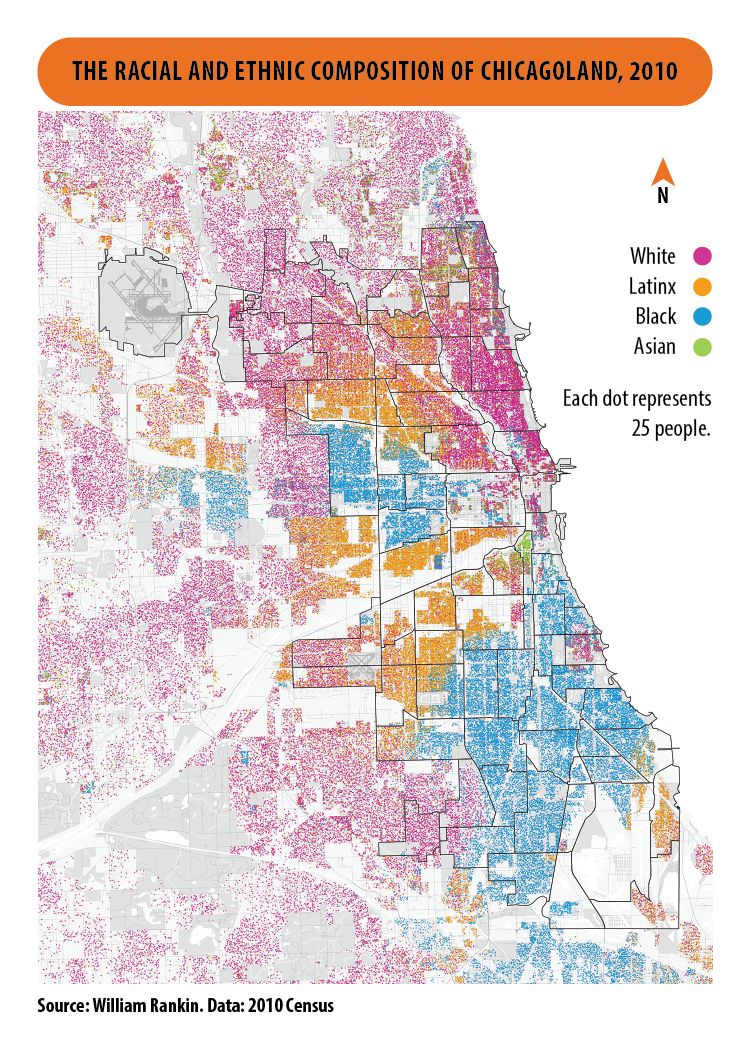
Residential segregation is a multi-scale phenomenon
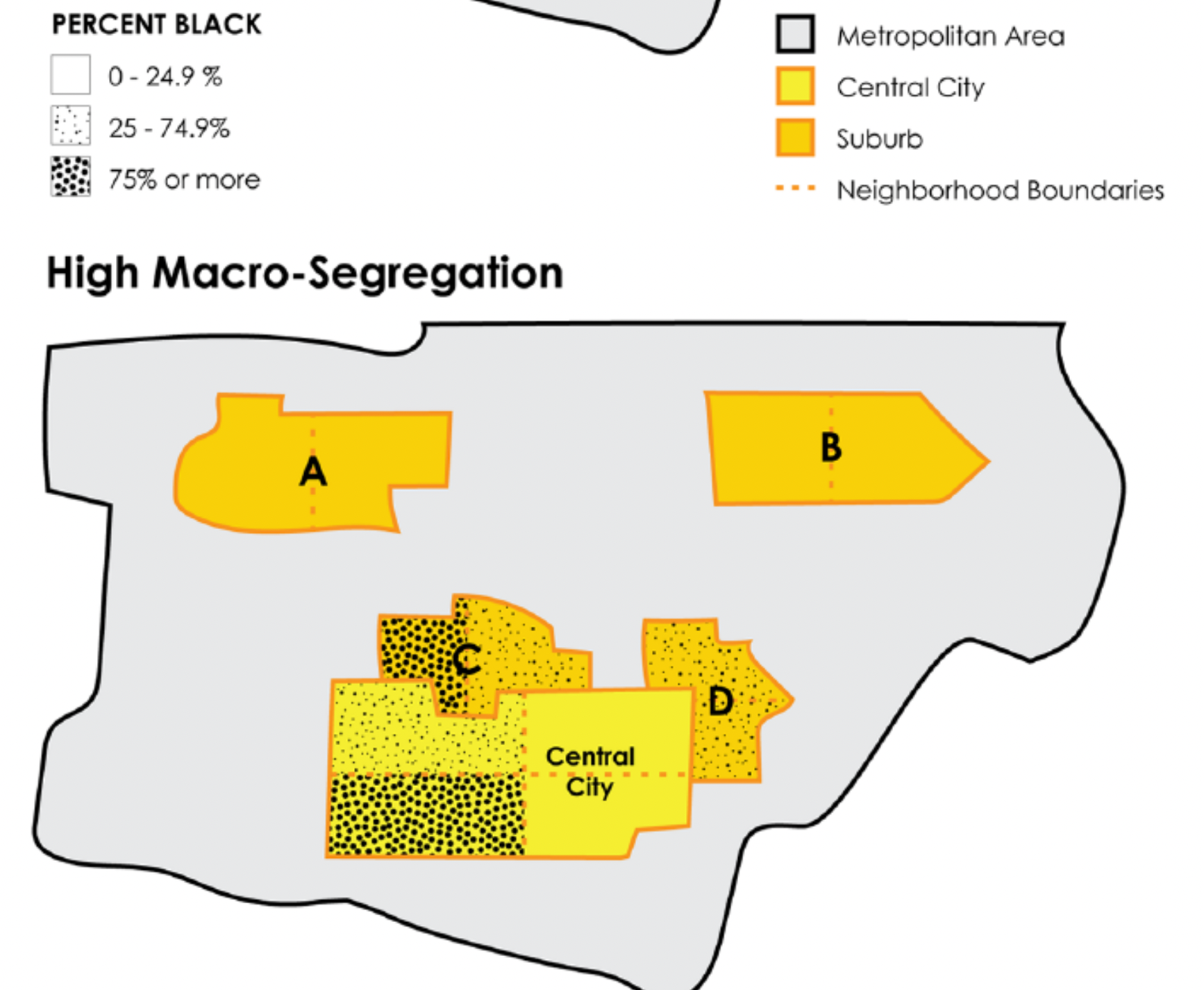
A Typology of Segregation
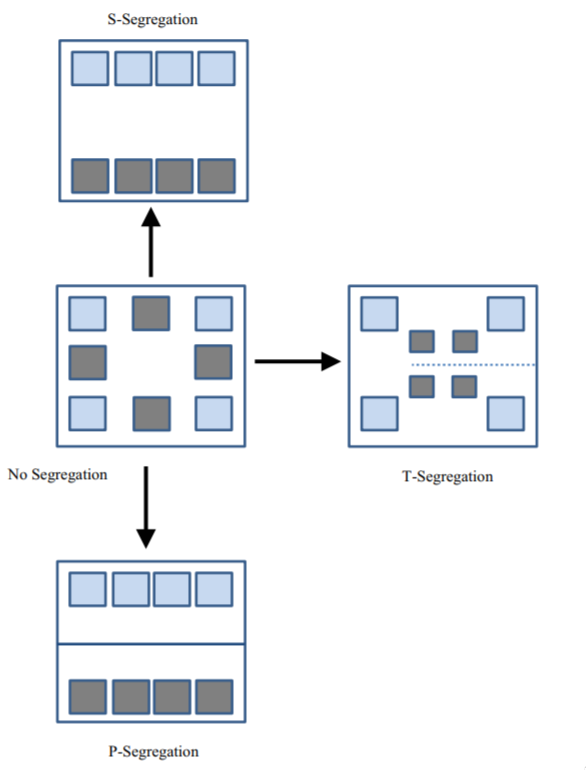
Clearly-defined primary segregation
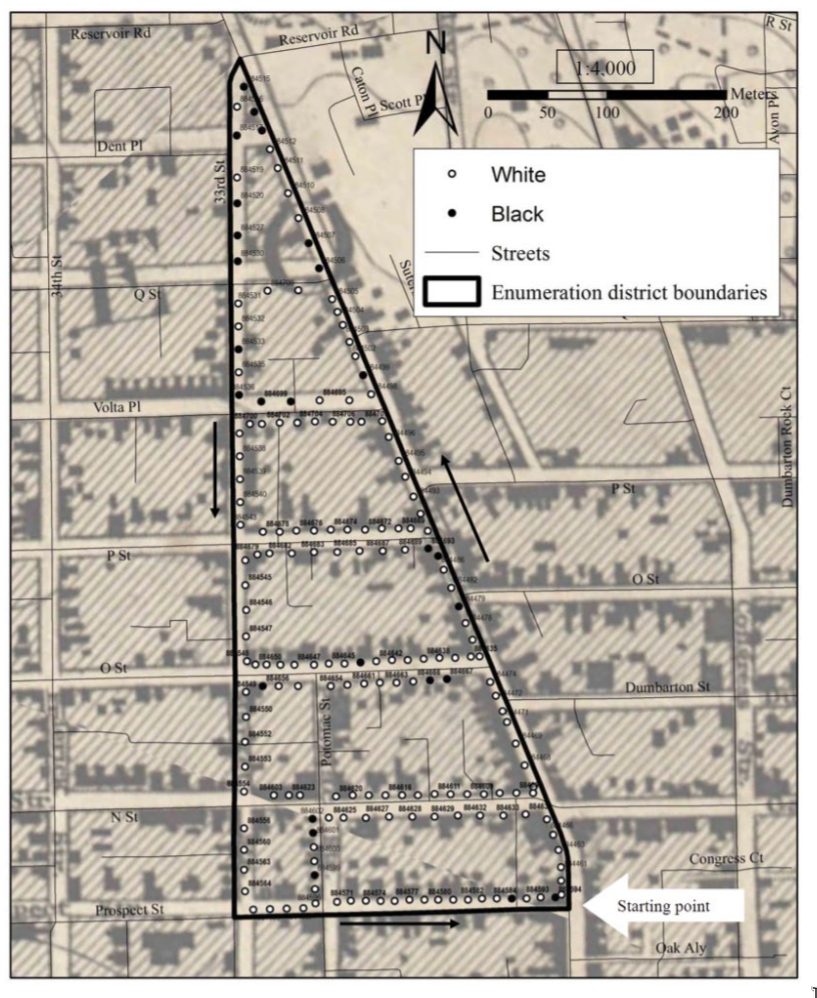
Fine-scale residential segregation in Washington, D.C. (1888)
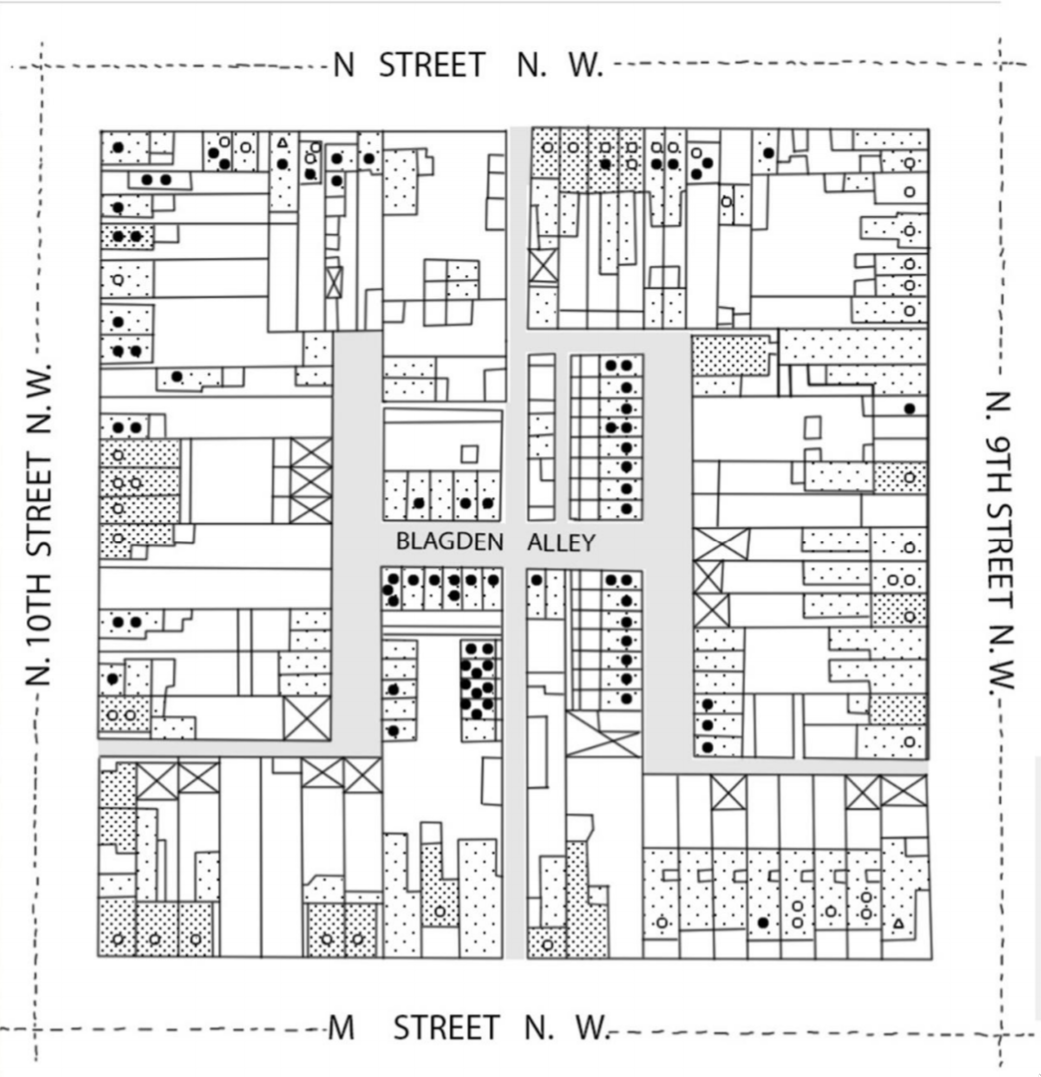
Sanborn Fire Insurance Company Map for Washington D.C. in 1888
Pattern was pervasive throughout D.C. and Baltimore
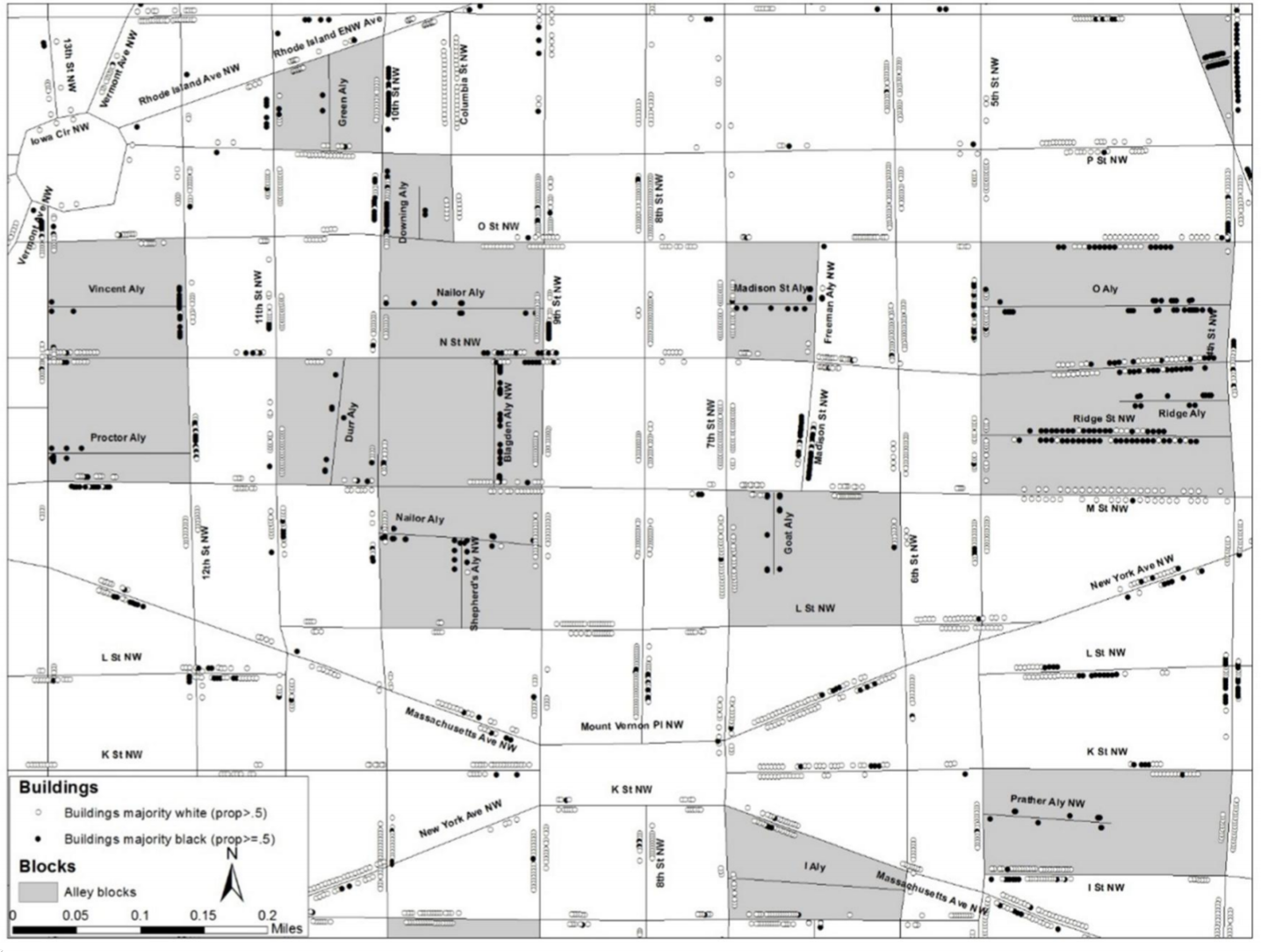
Map of a larger area of DC
What are potential implications of these different modes of segregation for infection risk?
So: How do we measure this type of segregation?
Classic approach, e.g. (Massey and Denton 1988), only captures primary segregation.
Grigoryeva & Ruef noticed that information could be extracted from the order in which 19th century census takers visited houses. (Grigoryeva and Ruef 2015)
Data were recorded sequentially in their records as they went 🏠 to 🏠.
Compared observed sequences of black and white households to a random distribution to measure the extent of tertiary segregation.
Called their measure the Sequential Index of Segregation (SIS)
Different measures \(\to\) different answers
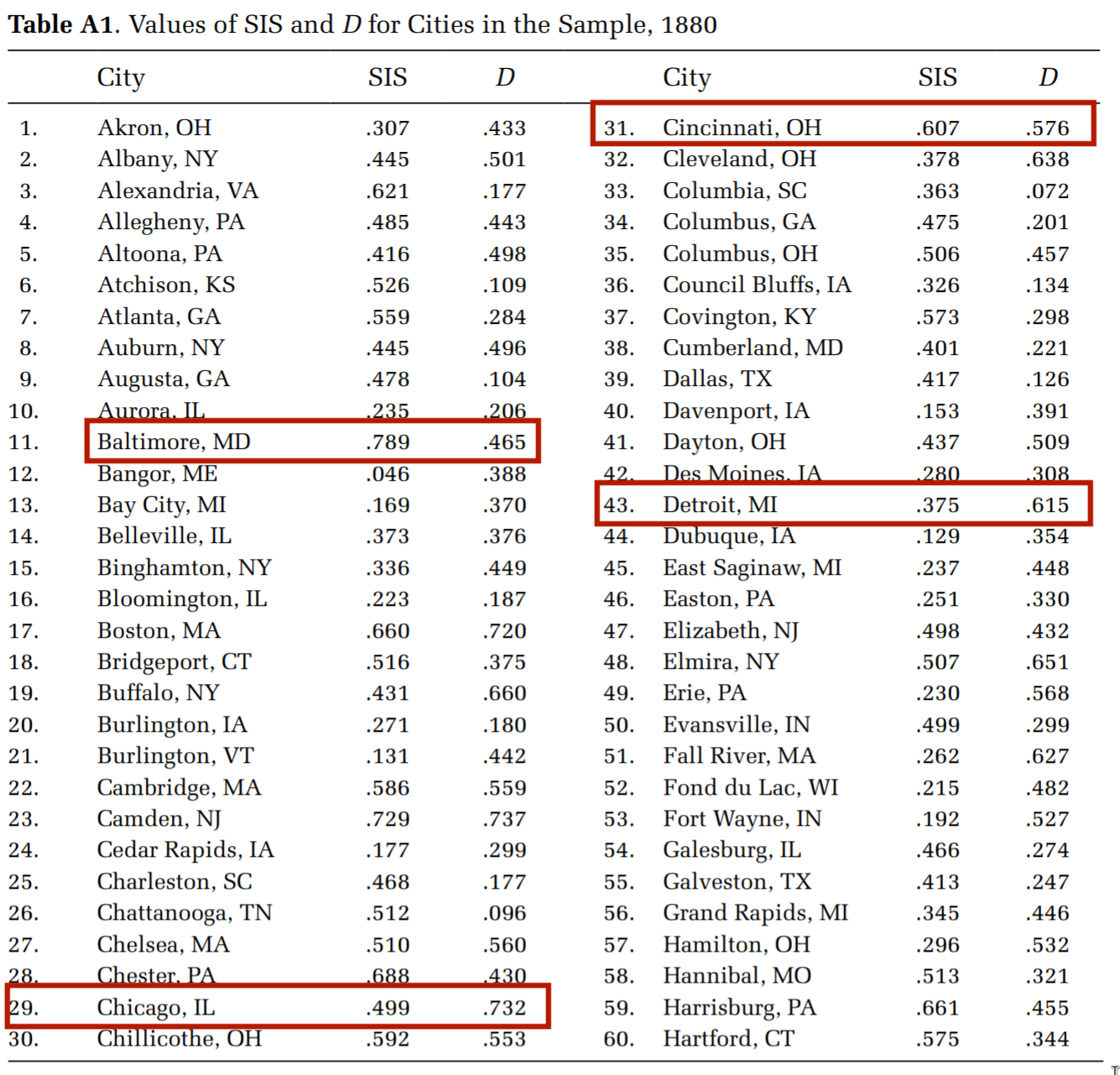
D = index of dissimilarity, a measure of evenness
What do you think this implies for how we should approach the measurement/characterization of segregation?
In pairs
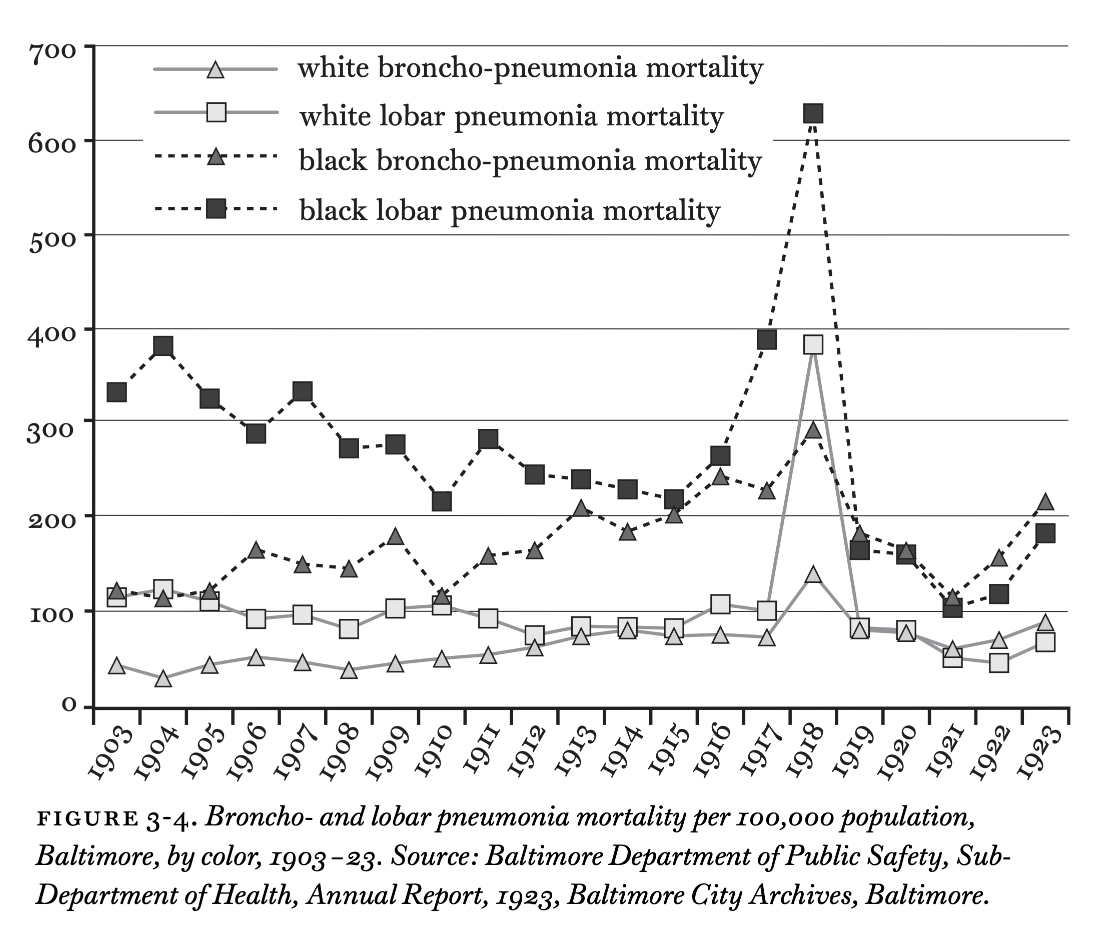
Focusing on Chapter 3, what does the discussion in this chapter add to our understanding of how segregation and racism act as fundamental causes of health inequality?
What other diseases - infectious and non-communicable - were linked to racial residential segregation and living conditions during the late 19th and early 20th centuries?
How does this information support - or not - the role of racism and SES as fundamental causes in TB disparities?
08:00
In groups of four
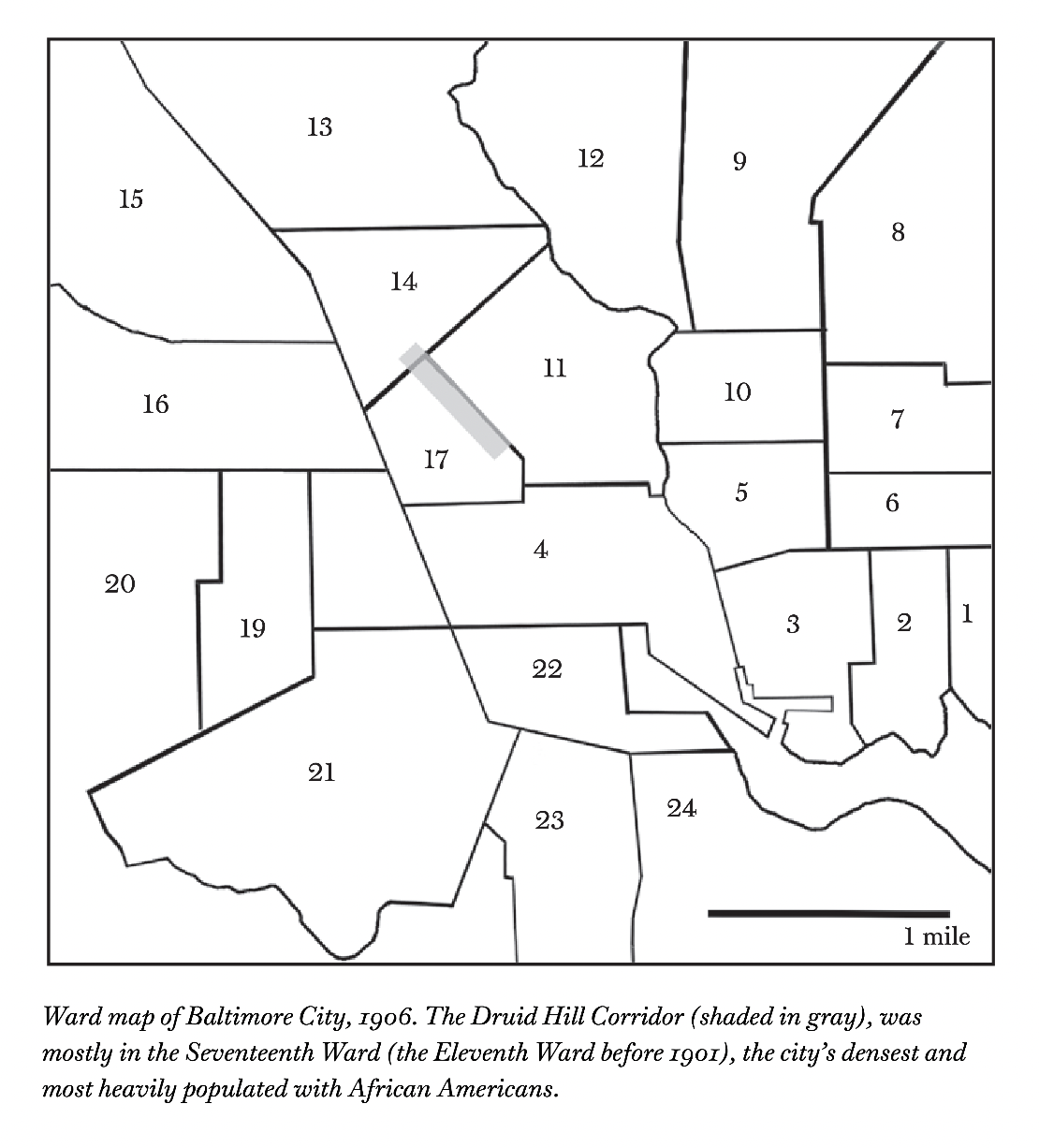
What are the push and pull factors that Roberts invokes to exlpain the emergence of the Druid Hill Corridor as a Black ghetto characterized by intense segregation and high rates of TB and other infectious diseases?
In chapter 4, what similarities and differences did you see been infected house theory and the miasmatic theories discussed in The Ghost Map?
- What were some surprising implications of infected house theory for public health surveillance and intervention?
10:00