Finding the Lung Block 🫁: Then and Now
PUBHLTH 405
Social Epidemiology of Infectious Disease
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
Conflating race and space
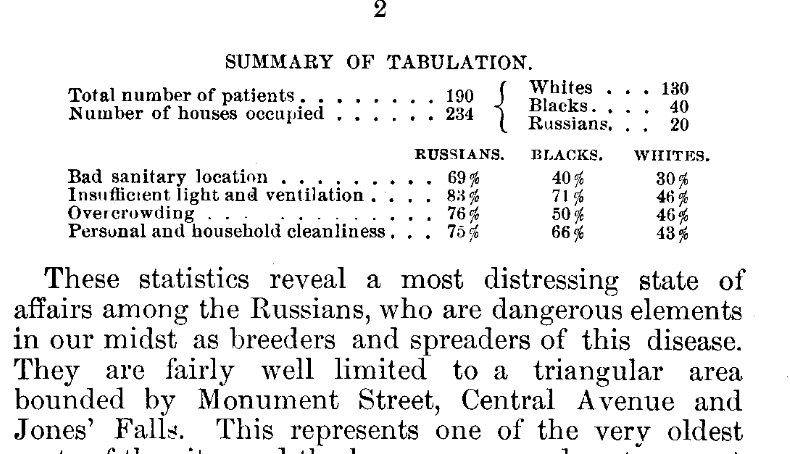
Adelaide Dutcher’s take on TB risk in Baltimore (Dutcher 1900)
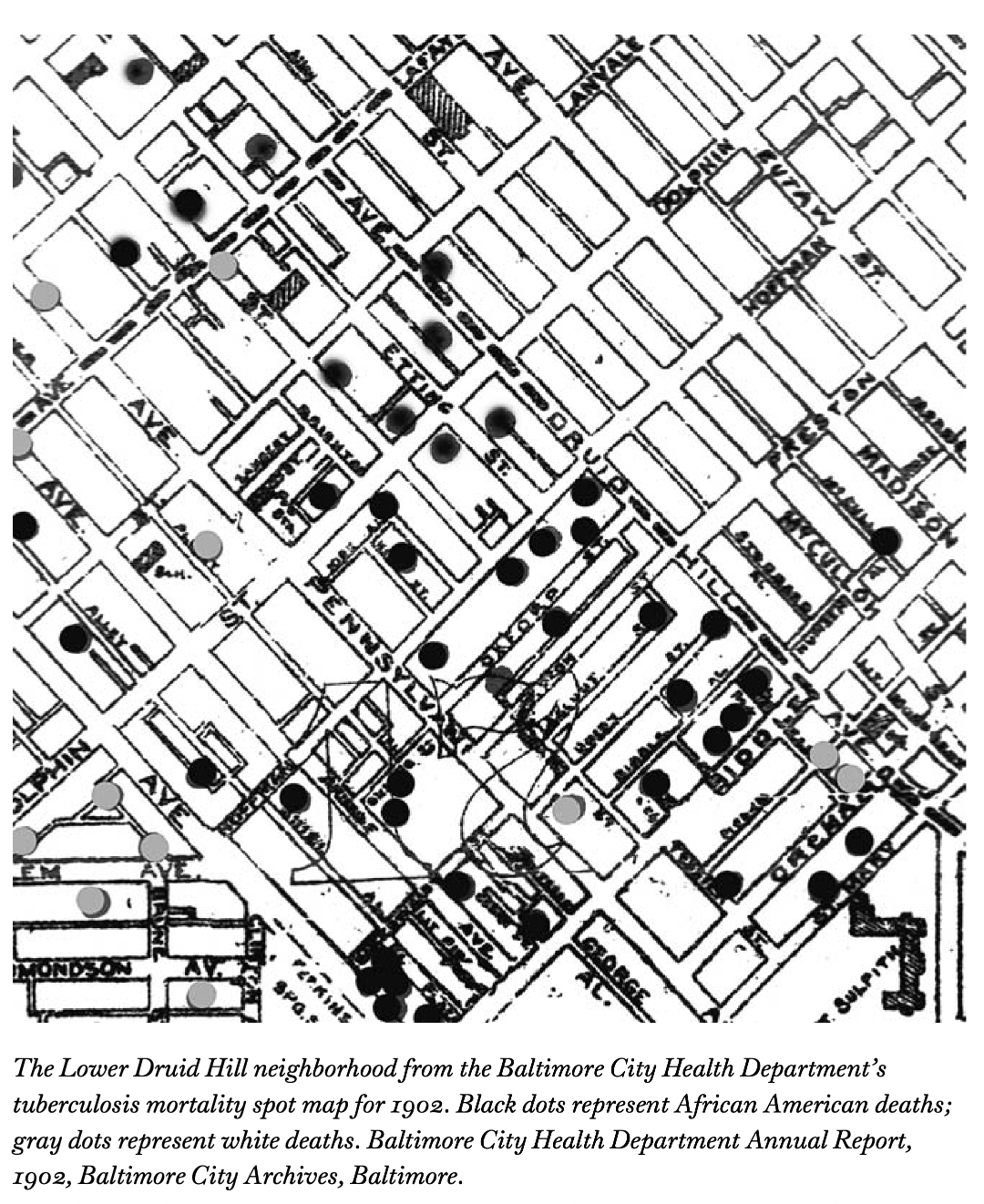
The Spot Map
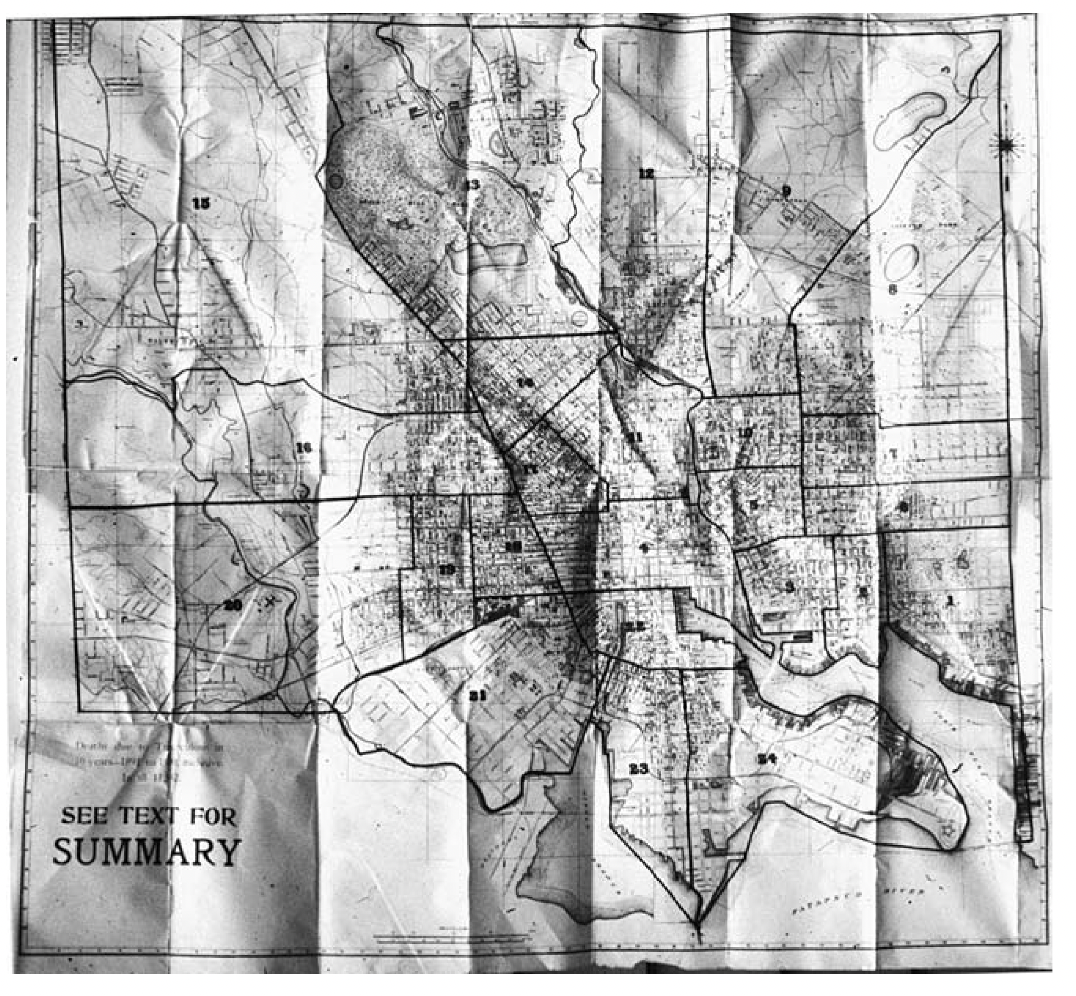
What is missing from the spot map that was present in John Snow’s Ghost Map?

Balancing the corners of the rhetorical triangle
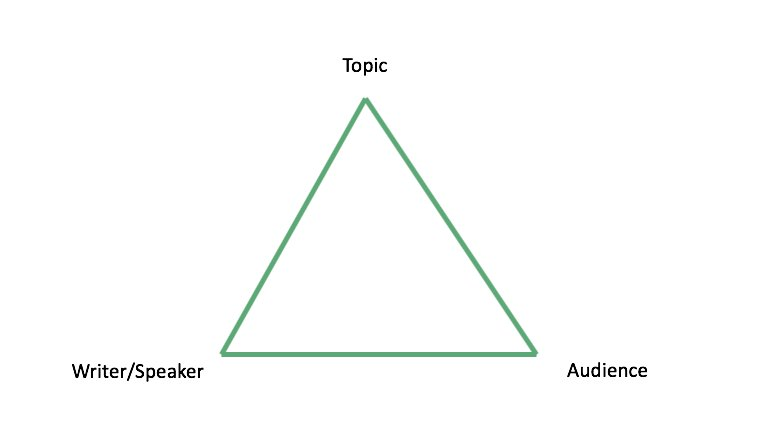
Effective communication reflects balanced attention to each element.
Challenge of the final assignment comes from metabolizing information and purposively communicating it to a new audience.
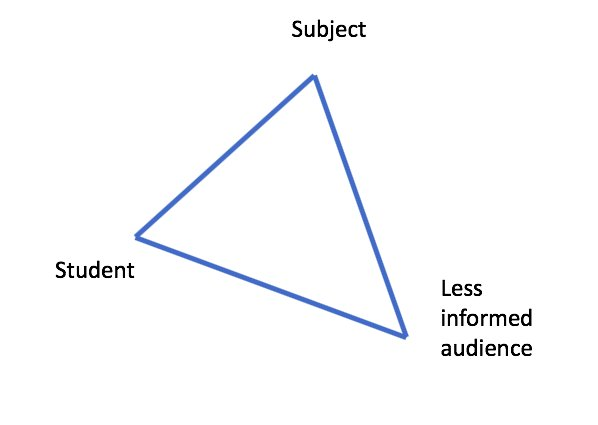
Starting with defining your communication goals and intended audience will help all the other pieces fall into place!