Making the Case
PUBHLTH 405
Social History of Infectious Disease
University of Michigan School of Public Health
Jon Zelner
[email protected]
epibayes.io
![]()
Today’s Theme
Who will win???
Small scale data provided compelling evidence for the droplet theory of SARS-CoV-2 transmission
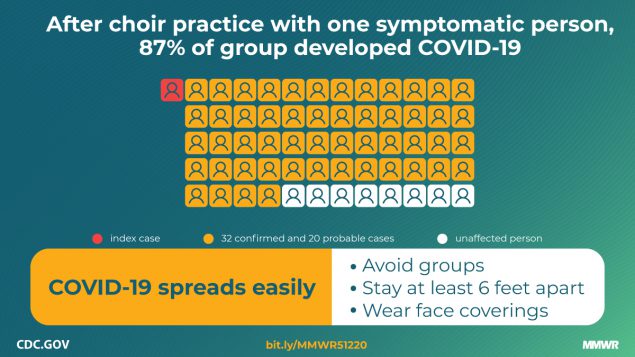
Does this bias against certain types of evidence echo anything from The Ghost Map?
Why didn’t mechanistic evidence dislodge the droplet-only perspective on SARS-CoV-2 transmission?
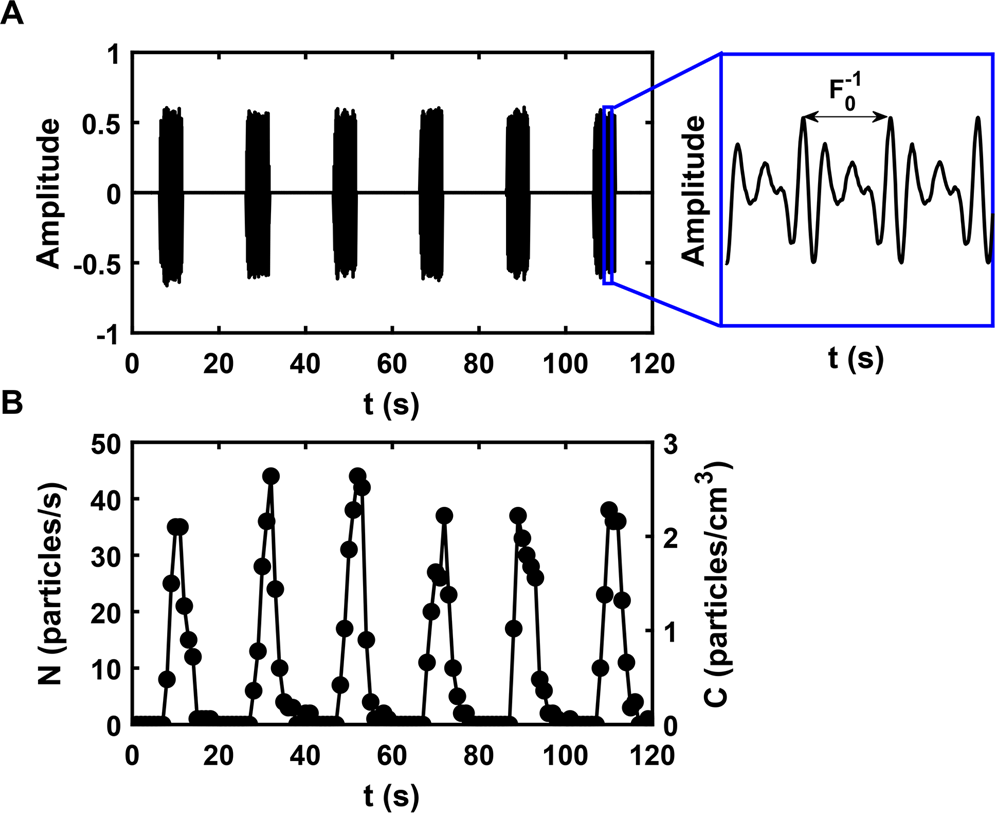
Relationship between voice volume and aerosol production (From Asadi et al. 2019)
EBM’s hierarchy of evidence
What is meant by ‘risk of bias’?
Quality of evidence?
Where would Snow’s explorations fit in this hierarchy?
How could you re-draw this hierarchy to allow for more consilient explanations?
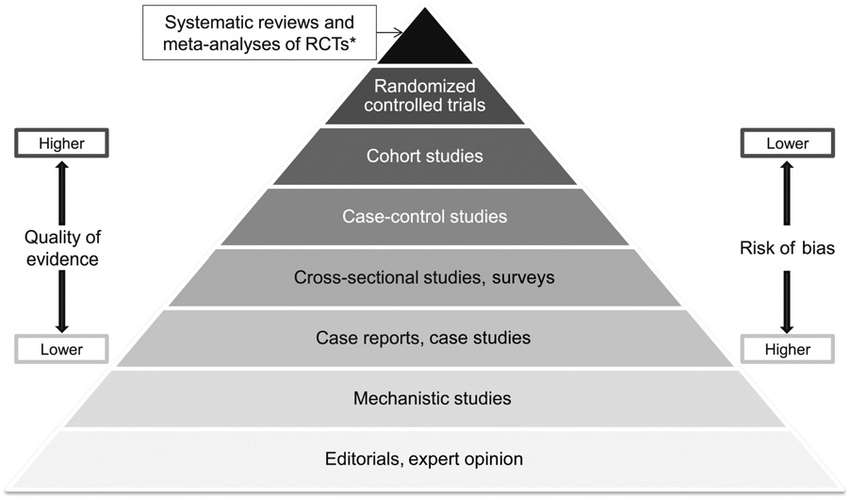
Why is this kind of diagram inevitably controversial?
Two ways of aggregating evidence


Where are we?
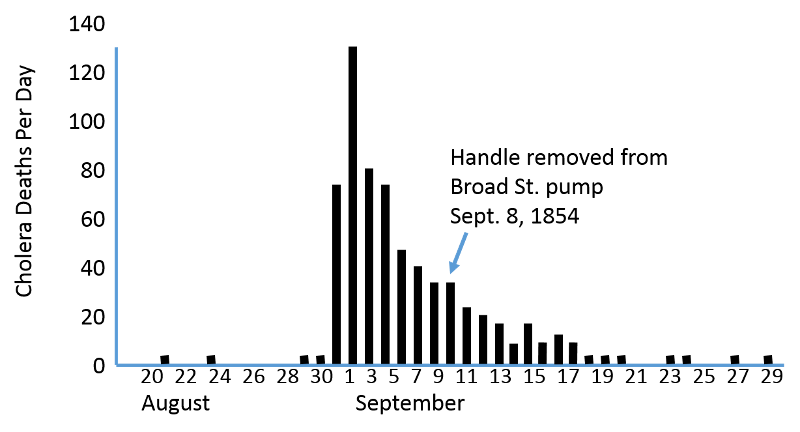
By September 7th, the outbreak had begun to subside prior to the removal of the pump handle on the 8th
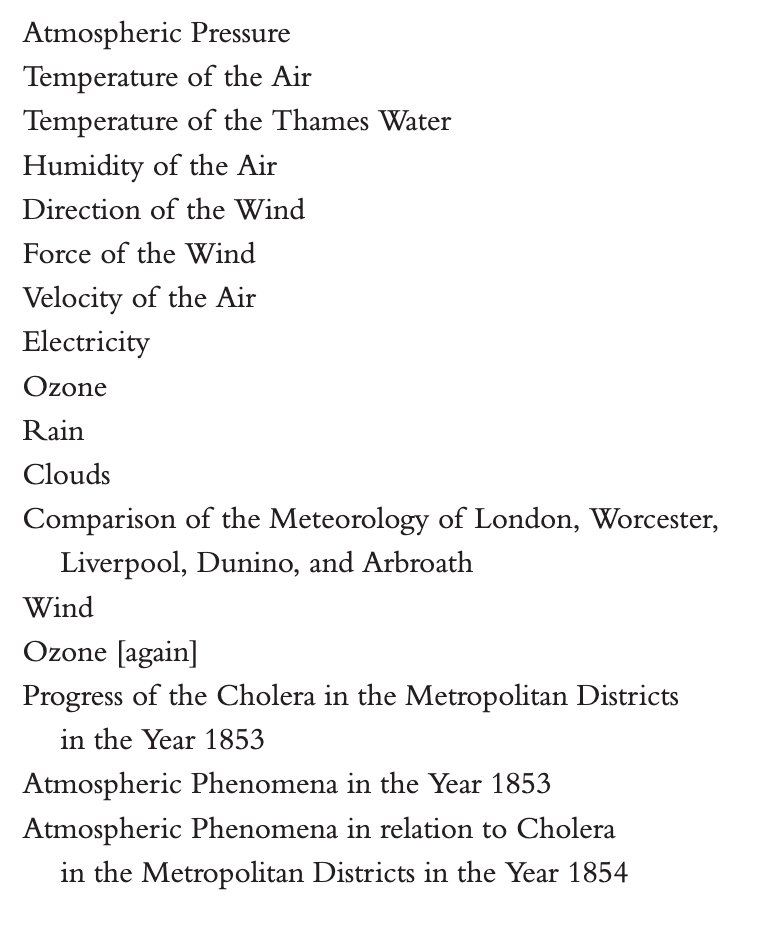
How did the Cholera Commission report deal with the evidence that Snow brought to bear?
The first map of the outbreak was not made by Snow
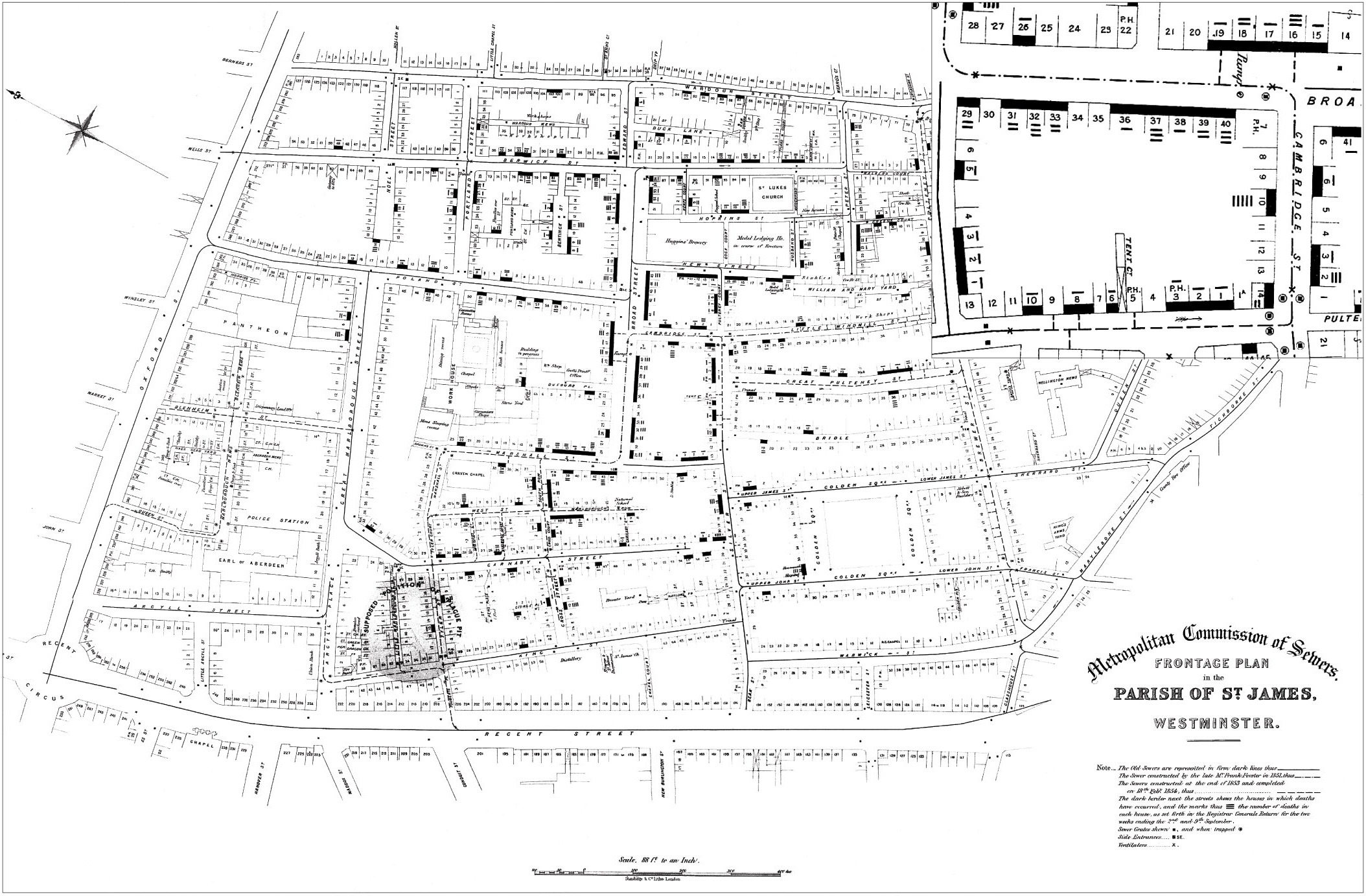
Edmund Cooper’s map of the locations of Cholera deaths relative to the location of a supposed ‘Plague Pit’ suspected of being the source of the outbreak
Snow’s first map made two crucial modifications to the layout used by Cooper
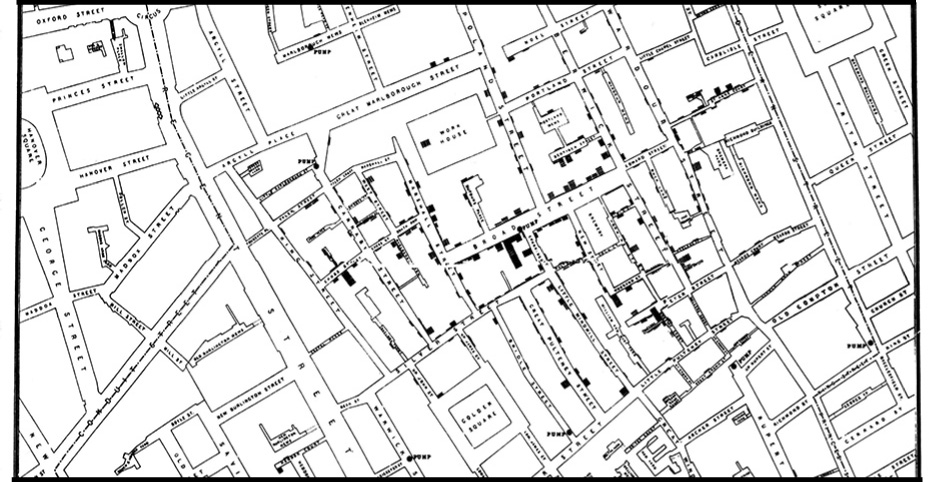
Snow’s bar map indicated the number of deaths at each location, the location of the pumps, and stripped away extraneous environental detail
A later edition of the map included another piece of information to push back on miasma

Snow traced a boundary indicating the locations for which the Broad Street Pump was the closest by walking time, showing that many deaths were clustered within this area.